Spousal Support as Experienced by People With Multiple Sclerosis: A Qualitative Study

Selected By
Colleen Harris, MN, NP, MSCN, MSCS
Why is this important to me?
Around 30% of people with MS require some type of assistance at home, and about 80% of that care is provided by family members, typically a spouse or partner. Features of MS such as severity, unpredictability, and limited effective treatment options are challenging to both the patient and his or her spouse. Although care provided is generally supportive and positive, sometimes the care can be problematic. Stress, which may sometimes be due to problematic care, is related to disease activity. The idea of “support” is broad and abstract and requires clarification. This study explored the complex phenomena of support provided by spouses of people with MS to increase understanding of spousal support in MS.
Who will benefit from reading this study/article?
People with MS who are married or in a committed relationship will benefit from reading this article.
What is the objective of this study?
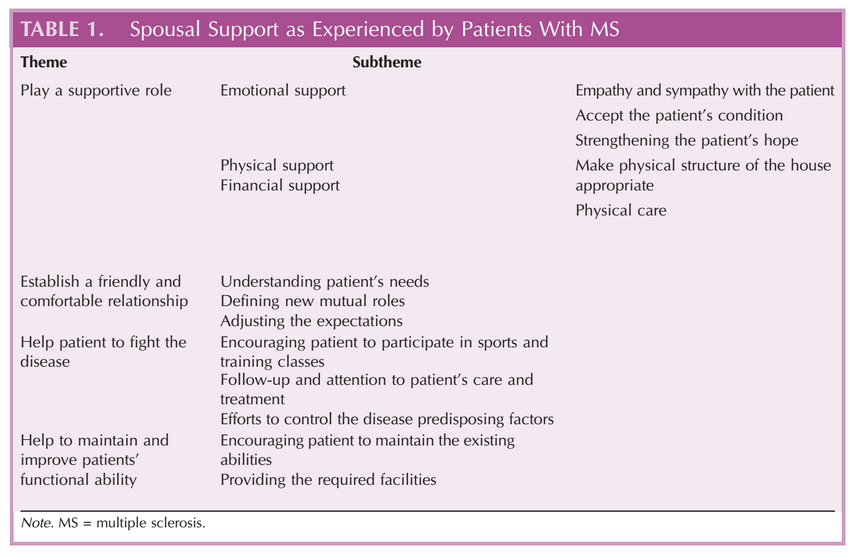
The investigators interviewed patients with MS and their partners, recorded the interviews, and explored their experiences. Four main themes for spousal support were identified:
- Spouses should play a supportive role. Three components of this theme were identified:
- Emotional support
- Physical support
- Financial support
Many patients felt that emotional support from their spouses was more important than physical assistance, but many spouses were unaware of this and believed that physical support was more important. Spouses also expressed a need for emotional support from their partner with MS. Overall, moderate help was preferred by patients so that they could maintain as much independence as possible. Other important features of effective support were sympathy, accepting the patient’s condition, and providing the patient with hope.
- Spouses should establish a friendly and comfortable relationship. Components of this theme were:
- Understanding the patient’s needs
- Defining new roles for each partner
- Adjusting expectations to reduce stress
An open, comfortable relationship enhances communication about problems, expectations, and needs.
- Spouses should help the patient fight the disease. Important components of this theme were:
- Encouraging the patient to participate in exercise
- Paying attention to the patient’s medical needs
- Controlling factors that worsen MS
Participants were aware that MS is manageable, and agreed that understanding the disease and factors that make it worse such as stress were important and made the patients less afraid and more willing to go on with life. Encouraging participation in exercise helped improve symptoms in many patients. Some male patients in particular did not take their medications as prescribed, and wives were able to help encourage medication compliance.
- Spouses should help to maintain and improve the patient’s functional ability. Important components of this theme were:
- Encouraging the patient to maintain his or her abilities
- Modifying the house and environment as needed to maintain independence
Maintaining existing abilities and helping to restore lost abilities were important goals. Patients expressed concern that an increased burden from caring for their partner with MS may lead the partner to leave the relationship, and that this loss of the relationship would be more painful than the disease.
In conclusion, receiving support from your spouse is very important for optimal management of your MS and for maintaining a good quality of life. Spousal support is one of the main types of support you may receive. Maintaining your independence as much as possible and providing support to your spouse will strengthen your relationship and may improve your MS. You may sometimes find that your spouse provides more support than you need. Open communication can help with adjusting needs so that both you and your spouse are satisfied with the level of care.
How did the authors study this issue?
The authors interviewed 25 married patients with MS and their spouses. Of the patients, 18 were women and seven were men. The average age of patients was 38 years, and they had been living with MS for an average of 9 years. Interviews consisted of open-ended questions such as “How did your partner help you adapt to your disease?”. Participants were encouraged to speak openly. Recurring themes were extracted from the interviews.
| SHARE: | |||||
For additional resources, visit:
Original Article
Spousal Support as Experienced by People With Multiple Sclerosis: A Qualitative Study
Journal of Neuroscience Nursing
Ghafari, Somayeh; Khoshknab, Masoud Fallahi; Norouzi, Kian; Mohamadi, Eisa
ABSTRACT: About 30% of people with multiple sclerosis require some form of supportive assistance at home, and 80% of that assistance is usually provided by spouses or partners. So, the explanation and understanding of patients’ experiences of support received from their spouses enable spouses and healthcare professionals to reform their actions toward positive support. This study aimed to explore the experiences of people with multiple sclerosis regarding support from their spouses. A qualitative content analysis method was used to conduct this study. The study participants were 25 patients with multiple sclerosis who were chosen through purposeful sampling from multiple sclerosis associations of Isfahan and Tehran (Iran). Data were collected through nonstructured interviews from September 2011 to August 2012. Four themes and nine subthemes emerged through data analysis. The main themes were play a supportive role, establish a friendly and comfortable relationship, help patient to fight the disease, and help to maintain and to improve patients’ functional ability. The results could help in improving the quality of spouses’ support in people with multiple sclerosis. Moreover, it could aid in determining the educational needs of patients as supported persons and spouses as supporters. The results could lead to increased knowledge of healthcare experts about the issue of how Iranian people with multiple sclerosis are being supported by their wives/husbands. Furthermore, it would help them to design caring models to promote successful supporting strategies for patients.
Multiple sclerosis (MS) is a chronic progressive degenerative neurological disease that demyelizes the central nervous system. In fact, it is thought to affect more than 2.5 million people worldwide (Gingold, 2011) and around 60,000 people in Iran. According to Iran Neurology Society, figures for people with MS have increased from 51.9 in 2009 to 73 in 100,000 people in 2011. In addition, prevalence rate of MS in Iran is 20 times higher than other countries in the region (Etemadifar & Sahraiyan, 2012). The MS is characterized by episodes of neurologic symptoms that are often followed by fixed neurologic deficits, increased disability, and medical and physical decline over 30–40 years (Buchanan, Radin, Huang, & Zhu, 2010); actually, it is the most common cause of neurological disability in young adults (Rudick, 1998; McKeown, Porter-Armstrong, & Baxter, 2003). The sociomedical model of the disablement process explains how chronic and acute conditions affect functioning in specific systems of the body, physical and mental activities, and daily life activities in young adults with MS. Furthermore, personal and environmental factors can speed up or slow down disablement of patients.
In this way, patients become limited not only in employment but also in educational opportunities or interpersonal relationships (Krokavcova et al., 2008; Roessler, Rumrill, & Fitzgerald, 2004). About 30% of people with MS require some form of supportive and maintenance assistance at home, with 80% of that care provided by informal or unpaid caregivers who are usually family members (Buchanan, Radin, Huang, et al., 2010). Previous studies have found that most informal caregivers of people with MS were the spouse or partner of the patient (Buchanan, Radin, & Chakravorty, 2009; Buchanan, Radin, Huang, et al., 2010). In fact, severity of the disease, unpredictability of its course, and lack of specific treatment bring a considerable challenge not only to the patient but also to the intimate partner. Along this way, beneficial effects of being involved in a supportive relationship for well-being in general as well as for adjustment to chronic illness have been well documented (Kleiboer et al., 2007). Unfortunately, besides being supportive, interactions with the partner can also be problematic and have detrimental effects of problematic or negative interactions, which are believed to be more important than the beneficial effects that are raised by supportive interactions (Newsom, Nishishiba, Morgan, & Rook, 2003). Because of their dependency, both of the couple are affected not only by their own reactions to the illness but also by the emotional distress of their partner (Rusbult & Van Lange, 2003).
Research has shown that there is a significant relationship between the well-being of patients and their partners; moreover, it often follows the same pattern over time (Segrin et al., 2005). In addition, for partners, taking care of an ill partner often implies taking additional responsibilities such as performing household tasks or assistance with self-care. Plenty of research has shown that taking care of an ill partner may be burdensome (Ybema, Kuijer, Hagedoorn, & Buunk, 2002). Thus, both patients and their intimate partners may lack resources to deal with stressful events and therefore may be psychologically vulnerable to any negative support that they receive from their partner. This notion of support was found in a study by Druley and Townsend (1998). Negative support that was received from the partner was related to depression through self-esteem in rheumatoid arthritis patients but not in healthy controls.
Moreover, for patients with MS, investigating support of partner is particularly important as it is suggested that stress (e.g., negative support) is related to periods of disease activity in MS (Newsom et al., 2003). Although support has been generally acknowledged as a critical factor in adapting to and coping with chronic illness, the mechanisms by which it influences the chronic illness experience are not yet well understood (Thorne et al., 2001). The concept of “support” is wide and is used in such diverse disciplines; however, the meaning of the phenomenon of spousal support as experienced by people with MS is not clear. Commonly, support is studied in terms of social support and as potential numbers of supporters. In MS, as a chronic disabling disease, spousal support is an important prognostic factor because of social isolation and patients’ physical and emotional declination (Nordgren, Asp, & Fagerberg, 2008).
A qualitative content analysis of unstructured interviews is used to explain and understand the experiences of individuals with multiple sclerosis (MS) relative to support from their spouses. The authors identify patterns that somewhat confound our usual expectations.
In fact, nursing research studies usually do not consider support as a spousal support, and the increased abstraction of the concept intensifies lack of clarity (Finfgeld-Connett, 2005; Williams, Barclay, & Schmied, 2004). If the details of such a concept as spousal support are not being defined in a particular context or do not reflect its meaning to people in the context, there may be problems assessing spousal support and undertaking interventions (Nordgren et al., 2008). The aim of the current study is to explore the exposal support experiences of the patients with MS. There are no other conducted studies that show the MS patients’ experiences of spousal support in Iran. Therefore, investigating their experiences of spousal support within the Iranian cultural context is critical and of great importance. For this reason, a decision was made to conduct a qualitative study, which is the most suitable method for determining the phenomenon of spousal support in people with MS (Polit & Beck, 2008).
Design
A qualitative study with a content analysis approach was used to investigate experience of spousal support of patients with MS. Qualitative research aims to explore the complex phenomena that are encountered by clinicians, healthcare providers, policy makers, and consumers in the healthcare system (Tong, Sainsbury, & Craig, 2007). It can be an important tool in understanding emotions and perceptions, and health policies can be developed through this type of research (Holloway, 2005).
Content analysis is a research method for making replicable and valid inferences from data to their context, with the purpose of providing knowledge, new insights, a representation of facts, and a practical guide to action (Elo & Kyngäs, 2008). In nursing research, content analysis is an essential way to provide evidence of a phenomenon, and qualitative research is considered to be the only way for the same purpose, especially in sensitive topics (Elo & Kyngäs, 2008). Content analysis is a systematic coding-and-categorizing approach, which can be used to explore unobtrusively a large amount of textual information to ascertain the trends and patterns of communication (Gbrich, 2007). This is perhaps the most common approach used in the qualitative research that has been reported in health journals. It aims to present the key elements of the respondents’ accounts. It is a useful approach for answering questions about the salient issues for particular groups of respondents or for identifying the typical responses (Green & Thorogood, 2004). According to the above, we decided to conduct a qualitative study with a content analysis approach for understanding emotions and perceptions of patients with MS about spousal support as a complicated phenomenon (Polit & Beck, 2008).
Participants
The participants in this study were 25 patients (18 women and seven men, aged 20–55 years) who had been experiencing MS for 4–26 years. They were selected through purposeful sampling method. The sampling done for qualitative studies is called purposeful sampling because it is directed by the purpose of the study, not by statistical calculations. According to the purpose of this study, we considered patients with MS who had the experience of being supported by their spouses and tended to talk of their experiences. The field of our study was the MS Society of Iran and neurologists’ clinics and rehabilitation centers that covered the participants. Participants were eligible for inclusion if (a) MS had been diagnosed for him or her for >=2 years, (b) patients were living together with their spouses for >=1 year, and (c) patients were willing to participate in the study without any problem in hearing and speaking and had no history of other pathological or chronic diseases.
Data Collection
The data were collected from September 2011 to August 2012 by means of unstructured interviews. Each interview lasted 50–90 minutes. The place of the interview was selected according to participants’ wishes. Each participant was interviewed one or two times (after transcription of some interviews, the researcher did not understand the meaning of participants, and another interview was necessary). Initially, the developed interview guide consisted of a number of open-ended questions, for example, “Would you please explain for me your relationship with your partner?” or “How did your partner help you to adapt to your disease?” Participants were encouraged to speak openly and to relate their personal experiences of support. Furthermore, as a part of the data collection process, field notes were used. Collecting data continued until saturation. In fact, data saturation occurred when a code or a new category did not emerge from data analysis (Strauss & Corbin, 1998). In this study, a saturation point was reached when no new data or category emerged after the interview with the 22nd participant.
Ethical Considerations
Approval to conduct the study was granted by the ethics committee of the University of Social Welfare and Rehabilitation Science in Iran. Potential participants were informed that participation in the study was voluntary, they could withdraw at any time, their confidentiality would be maintained, and no individual would be identified in any publications arising from the study.
Data Analysis
Qualitative content analysis was used for analyzing data (Sandelowski, 2000). In this way, recorded interviews were transcribed verbatim by the primary author (S.G.), and then two of the researchers (S.G. and M.F.K.) read the transcripts independently to obtain a sense of the whole. The text was extracted into condensed meaning units that were abstracted and labeled with a code (S.G.). After that, various codes were compared based on differences and similarities and sorted into categories and subcategories, which made up the manifest content (S.G.). The tentative categories were discussed by three researchers (S.G., M.F.K., and E.M.). Finally, the underlying meaning, or the latent content of the categories, was formulated into themes by three researchers independently (S.G., M.F.K., and E.M.) and then compared and contrasted until agreement was reached.
The following steps were taken to analyze the data (Granheim & Lundman, 2004):
1. Transcribing the interviews verbatim and reading through several times to obtain the sense of the whole.
2. Dividing the text into meaning units that were condensed.
3. Abstracting the condensed meaning units and labeling with codes.
4. Sorting codes into subcategories and categories based on comparisons regarding their similarities and differences.
5. Formulating themes as an expression of the latent content of the text.
Validity and Reliability/Rigor
Initial themes were carefully reviewed by the study team. Credibility increased through member checking and validation of emerging codes and categories in subsequent discussion and through comparing and contrasting by three researchers (S.G., M.F.K., and E.M.) until agreement was reached. The conformability and credibility of the findings were verified through member checking, peer checking, and maximum sampling variation. To create intertranscript reliability, two experts conducted the second reviewing process. About 70% of the codes and categories were revised to the point at which the study team expressed strong agreement. To reach a conclusive decision, disagreements were modified by discussion.
Findings
Participants in this study were 25 patients: 18 women and seven men, with a mean age of 38 years and a mean of 9 years experience of the disease; two patients were with master’s degree education, six were with bachelor’s degree, four were with associate degree, six were with diploma, and seven had under diploma education. In addition, all participants were married and living with their spouses for >=3 years.
During data analysis, four main themes and nine subthemes emerged from the experiences of the spousal support of patients with MS (Table 1).
Play a Supportive Role
Emotional Support
All participants believe that emotional support of their partners is more effective than their physical help and support in coping with the disease. Several female patients reported the need for emotional support from their husbands.
P4: “My husband tries to do my chores, to cook, to clean house, but for me the emotional support is more important than physical assistance.” [woman, aged 34 years]
Only one male patient reported not receiving emotional support from his wife.
P1: “My wife did not understand me! I needed more emotional support than physical assistance, but she was just taking care of me physically.” [man, aged 41 years]
Empathy and sympathy with the patient
Most participants believe in sympathy of their partners as an effective item in eliminating conflicts, making the right decisions for solving the problems, which are caused by disease, boosting confidence, and getting rid of loneliness and desiring to participate in societal and group activities.
P22: “My spouse understands my feelings so well, sometimes I cry hard because of my disabilities but he embraces me and sympathizes with me.” [woman, aged 38 years]
Accept the patient’s condition
Because participants did not always feel accepted by their wives/husbands, this aggravates their own skepticism about themselves, but when their spouses were accepting of their condition with MS, their confidence increased, and as a result, they tried their best to adapt to the disease. In this study, it is interesting that the fear of not being accepted with MS by spouses was equal for men and women. However, women were more supportive toward their husbands.
P21: “I’ve always thought that my husband no longer loves me because of my disease and my inabilities, but he told me: I accept all that you are. He asked me to go to a studio to take a photograph once again after our marriage. My doubts about our love were completely eliminated.” [woman, aged 34 years]
Strengthening the patient’s hope
For a patient who does not know the hardships ahead, hope is crucial. Participants believed the role of their partners is vitally important to continued living.
P19: “My husband kept telling me: do not even think about your disease, think about having a baby together and going out. He always finds something to make me hopeful about the future.” [woman, aged 49 years]
Physical Support
There is no doubt that a patient with MS needs cyclical or permanent physical assistance because of MS and disabilities because of physical health problems. All participants reported the role of family and spouses as being very important in this case.
Make physical structure of the house appropriate
Sometimes, spouses try to make changes in the home structure to help patients cope with their disabilities.
P3: “My husband bought me a chair with a brake and an outside the bath tub shower and installed some knobs in the bathroom and in the house. Moreover, he removed all additional items in the way from the bedroom to the bathroom.” [woman, aged 51 years]
Physical care
A number of participants who had physical disabilities were being cared by their spouses. The following transcription is a part of the researcher’s observations in this regard:
P12: “My husband took me to the clinic of occupational therapy 3 times a week with a wheelchair. Sometimes, in the middle of therapy sessions, I had problems because of my inconsistency. At these times, my husband entered and took me to the bathroom and washed me.” [woman, aged 39 years]
P22: “In the hospital, my wife dressed me and assisted me in going to the toilet and doing my personal hygiene, if she had not been there I don’t know what I would have done.” [man, aged 42 years]
Financial Support
All participants were exhausted because of the high costs of medications and hospitalization and the fact that the bulk of these costs are not covered by insurance. In this way, families and partners play a major role in paying the costs.
P14: “I know that the costs of drugs, herbs, and healthy foods is too much, but my husband provides all of them as far as he can and he doesn’t mind at all.” [woman, aged 35 years]
Establish a Friendly and Comfortable Relationship
According to the experiences of the participants in this study, having an open and comfortable relationship with their spouses enabled them to talk together about their problems, expectations, and needs and to agree on these kinds of issues. If they could not speak about these matters easily, they could never achieve balance and tranquility.
Understanding the Patient’s Needs
Spouses of some of the participants had attempted to establish a relaxed relationship with their husband or wife; in fact, they encouraged them to talk about their concerns and needs.
P6: “My husband treated me so comfortably that unconsciously, I became like him, free of any embarrassment or obstruction, I tell him my physical and psychological needs. Actually, our relationship is very friendly and free of any stress.” [woman, aged 48 years]
Defining New Mutual Roles
Experiences of the participants in this study indicated that illness and disability cause difficulties in performing their roles. Moreover, it makes some changes compulsory in the roles of couples. More precisely, these changes only happen within a comfortable relationship rich in trust.
P18: “I try as much as possible to continue my previous responsibilities. My husband interacts with me in a comfortable and close relationship. For example, he helps me in taking care of the children; he sometimes cooks food and does the laundry.” [woman, aged 45 years]
Adjusting the Expectations
Some participants pointed to the fact that their partners tried to reduce the patients’ stress by adjusting their expectations.
P2: “My husband didn’t expect me to prepare food or iron clothes on time, he told me act as you like I trust in your efforts.” [woman, aged 39 years]
P16: “My wife told me, I do not expect you to do as before or to take us on vacation. I just want you to try to get better.” [man, aged 44 years]
Help Patient to Fight the Disease
Most participants were convinced that MS is manageable. In other words, it is possible when you know how to deal with it and do it properly. In this study, an important step in fighting MS was understanding the disease and its predisposing factors.
Encouraging Patient to Participate in Sports and Training Classes
Because of spouses’ encouragement, many patients participated in yoga or swimming classes to control and improve symptoms of the disease.
P9: “Because my husband encouraged me, I attended yoga classes, which were very effective in calming my soul and helped relax my muscles.” [woman, aged 47 years]
Furthermore, spouses’ attempts to explain MS to the patient was especially helpful in the fight against the disease.
P15: “He tried to explain the disease to me. He encouraged me to participate in the training meetings of the MS society. Moreover, he bought me some books. At first, I did not accept and resisted, but he was so insistent. In this way, when I had gained a better understanding of MS, I was less afraid and more willing to continue my life.” [woman, aged 41 years]
Follow-Up and Attention to Patient’s Care and Treatment
In this study, some of the male patients did not heed their medical treatments, and their wives were more careful in this case. According to the patients themselves, it is just because of their disgust with the issue of acceptance of disability and drug dependency.
P17: “I did not care about my medications at all, but my wife was so careful about my injections and tried to inform me about proper and punctual use of my medications.” [man, aged 34 years]
Efforts to Control the Disease Predisposing Factors
Some patients express that their spouses try to take some predisposing factors away from them.
P11: “My wife tried to take me away from stressful environments. She eliminated animal fat from my diet; moreover, she kept the home temperature moderate. If the kids had any problems, she did not tell me so as to avoid increasing my stress.” [man, aged 38 years]
Help to Maintain and Improve Patients’ Functional Abilities
According to patients’ experiences, their partners used various methods to reconstruct and improve their lost abilities and to improve their existing abilities. Encouraging the patient to maintain the existing abilities and providing the required facilities were the best strategies that were used.
P8: “My husband told me: you should try to do your work and whenever you need me I’ll be there. He brought the kitchen cabinets down lower. He removed the sink to put a wheelchair there so I could do the cooking and wash the dishes.” [woman, aged 39 years]
P24: “My wife told me: although your hand and right foot are numb, you still have lots of abilities. You should try to do your work and not be dependent on me or your friends.” [man, aged 35 years]
P10: “My husband bought me a wheelchair with brakes and installed multi knobs to the walls of the bathroom so I could shower—with great difficulty, but alone. I was so happy. I should not be dependent on anyone. I still have lots of abilities.” [woman, aged 42 years]
Participants believed that, after a while, loss of functional independency will increase the workload of spouses and make them tired, and it is probable that they may leave their wives/husbands—something that would be very painful to the patient.
P2: “I try to maintain independence in doing my daily tasks. It is very painful for me to think that my husband might leave me due to his high workload.” [woman, aged 39 years]
P5: “If I can’t maintain my functional independence, someday he will be exhausted from the high workload and leave me. For me, it is more painful than the disease.” [woman, aged 44 years]
P11: “I know that my wife will finally be exhausted from doing all these works and responsibilities and leave me. It is really painful. I wish I could do my tasks and responsibilities alone; she is really under pressure from doing more work.” [man, aged 38 years]
Discussion
To the best of our knowledge, this study is the first qualitative research describing experiences of spousal support of people with MS. The findings of this study share similarities and differences with other researches carried out about patients’ support by caregivers, especially spouses’ support in MS and other chronic diseases. In fact, the partner relationship is generally thought to be one of the most important resources of social support, because of the fact that the partner is the main person who provides emotional and instrumental support (Bisschop, Kriegsman, Beekman, & Deeg, 2004). Similarly, the effects of perceived social support have been the most frequently examined, especially the effects of perceived emotional support (beliefs that love and caring, sympathy and understanding, esteem, and value are available from family members; Thoits, 1995).
To deal with MS, patients may need increasing amounts of both instrumental help and emotional support from their partners. Because of the physical disability associated with MS, it is likely that patients receive more physical help (Kleiboer et al., 2007), but participants in this study had a different view—they knew emotional support from their spouses was more important than their physical assistance. However, many partners were unaware of this issue and were supporting patients more physically. Interestingly, according to a number of participants, their spouses had the same need, emotional support from patients; spouses of patients said that continuing care without getting emotional support from patients is almost impossible. Several studies have shown that support received from the care recipient may buffer the negative consequences of care giving. For example, Wright and Aquilino (1998) found that reciprocity of emotional support between care giving wives and husbands who received care was linked to lower levels of burden among these wives.
About the physical assistance, participants said that physical moderated help is better, because too much assistance from their caregivers plus numbness, weakness, and fatigue of the disease caused them to be dependent. Patients were concerned that their spouses become tired of care and, for this reason, tried to maintain their independency. Fisher, Nadler, and Whitcher-Alagna (1982) and Gleason, Iida, Bolger, and Shrout (2003) referred to this issue and said: support and help from others often contain a mixture of enhancing and threatening elements. On the one hand, support may communicate that one is loved and cared for. On the other hand, it may signal that one has failed, which caused dependency of the person who received support.
However, participants in this study understood that physical support from their spouses was very effective in coping with new situations. In this study, participants received physical support from their spouses often as developing necessary facilities to perform household chores or helping to do personal tasks. Also, in this study, physical care was another kind of physical support of patients with disabilities and other problems caused by the disease. In the study of Schwartz and Kraft, people with MS were interviewed over the telephone, using standardized questionnaires to assess patient physical and psychological functioning, spouses’ responses to patient disability and good behaviors (i.e., “How does the spouse respond when you’re having difficulties related to multiple sclerosis?”), and family environmental factors. Forty-four patients with definite MS participated in the study. The findings of the Schwartz and Kraft study showed that most patients received physical support from their spouses, and this assistance, for the most part, was in the form of physical care and cooperation in performing the tasks of the patients (Schwartz & Kraft, 1999).
In this study, 18 women and seven men participated. The experiences of the participants indicated that only one of seven men did not receive any support from his wife, but of the 18 women, six were not supported by their husbands. This proportion suggests that more men than women were supported by their spouses, both emotionally and physically. On the basis of our knowledge, this finding was concluded less in studies abroad; therefore, it could be related to cultural factors and nursing and compassionate morals of women as well (Dalkhmoosh & Ahmadi, 2013; Ehteshamzade, 2009; Stambor, 2005).
One of the experiences of patients in this study was comfortable and open relationship with their spouses; to be precise, participants said that this relationship had caused them to talk with their partners about their needs comfortably, even sexual needs with no embarrassment. Furthermore, caregivers who are spouses or partners usually face changes in their sexual relationship. These changes can have physical or emotional causes. Furthermore, MS can interfere with both sex drive and function. In addition to MS-related functional problems, changes in roles may change the sexual relationship. In other words, caregivers feel that they are performing a parental role, rather than being a lover or a spouse; unfortunately, this could dampen intimacy (Radford, 2011). In a similar way, Benedict et al. have confirmed this issue. In their study, 70 people with MS and their spouses participated; researchers said that, in the relationship between patients with MS and their spouses, comfort and freedom of both in expressing feelings, expectations, and problems had been the main keys to living together with MS (Benedict et al., 2009).
This friendly and comfortable relationship had caused spouses to express their expectations and needs to the patients in a manner in which an equilibrium of expectations, responsibilities, and roles was brought into existence to continue their routine life. Radford wrote in her book that MS is extremely changeable and unpredictable. More precisely, people experience attacks and remissions, loss, and recovery or partial recovery of abilities. For instance, 1 day, a person with MS can dress alone; the next day, the person cannot. In this way, the caregiver has to take and then give back responsibility for tasks all the time. Actually, caregivers will need to rethink tasks and family schedules to ensure the smooth running of the roles (Radford, 2011). Almost half of the participants had experienced open communication and friendship with their spouses and knew it as an effective factor for coping with diseases. Therefore, educating patients with MS and their spouses about how their relationship should be seems necessary. Furthermore, conducting other researches about the impact of the relationship between patients and their spouses on adapting to the disease seems advantageous.
Most of the participants mentioned that helping the patient to fight the disease and preserving and promoting his or her functional independency were other kinds of support by spouses. In a study by Kleiboer et al., which was performed on 61 people with MS and their partners, it was determined that coping with the disease and trying to maintain abilities would not be possible just by patients’ efforts—the encouragement and support of spouses are crucial in this way (Kleiboer, Kuijer, Hox, Schreurs, & Bensing, 2006). As an example, one of the actions that spouses did to help patients to fight the disease was paying attention to and following up medical care. Some participants, most of whom were men, expressed that fatigue caused by constant use of drugs and lack of cure caused discouragement and discontinuation of the treatment. However, most often, their spouses had encouraged them to take the medication and visit their doctor regularly. Because of psychological reasons, men see themselves as being stronger than women (Simon & Nath, 2004; Taylor, Morin, Cohn, Clark, & Wang, 2008), so they do not accept dependence on permanent medication; as a result, attention and psychological care of patients to accept the disease and treatment appears to be essential. Several studies, such as Janssens et al., Dennison et al., and McCabe and Di Battista, considered a number of factors as coping factors in the fight with MS, such as attempt to gain information about the disease, exercise, follow the treatment, and control of disease’s predisposing factors such as heat and stress (Janssens et al., 2003; Dennison, Moss-Morris, & Chalder, 2009; Dennison, Moss-Morris, Silberb, Galeac, & Chalder 2010; McCabe & Di Battista, 2004).
In fact, none of the patients in this study had a tendency to be dependent on their families and so tried to keep their functional independency as much as possible to live with their spouses peacefully. In other words, participants in this study believed that, after a while, loss of functional independency will increase the workload of spouses and make them tired, and it is probable that they may leave their wives/husbands—something that would be very painful to the patient. Some of the participants in this study were very pleased with their spouses for encouraging and helping them to maintain and promote independency for doing personal tasks and responsibilities. Buchanan et al. (2009), McKeown et al. (2003), and Kleiboer et al. (2006) mentioned that spouses’ and other informal caregivers’ attention to maintain patients’ independency while helping them is of paramount importance. In addition, some participants were unhappy with their spouses because of too much physical assistance and their own limitations;in fact, they saw this as a factor in losing their remaining capacity. Therefore, providing education to informal caregivers by healthcare experts about the sufficient amount of help and support appears to be necessary. There is no provision of paid care in Iran, and the families bear the burden of care because of the great dedication and cordiality that exist among family members; therefore, support of families through the care of patients is very important (Shamsaei, Mohamad, Kermanshahi, & Vanaki, 2012). One of the limitations of this study was assessing only patients’ experiences; despite this, it is better to consider the experiences of spouses’ support in people with MS. Considering that most participants were women, more experiences belong to them, and this can be another limitation of this study.
Conclusion
On the basis of our findings, it is better to consider some items for planning and appropriate supportive care and educational programs. First, based on the experiences of patients with MS, despite having physical disabilities, patients need emotional support more than physical support; however, spouses supported the patients more physically than emotionally. Second, understanding the patient’s needs, defining new mutual roles, and adjusting the expectations were other main points of support, which were experienced by patients and are necessary factors to continue to share a life despite having a chronic debilitating disease. According to the experiences of the participants, the latter would not be possible to achieve except through establishing a friendly and comfortable relationship. Third, participants did not consider their chores being done by their spouses as a supportive action, but they experienced that their spouses’ attempt maintained and enhanced their independency in functioning as a positive supportive action. A number of spouses did not support patients moderately; they helped too much. Furthermore, in this study, men were supported by their spouses more than women. This could be related to cultural context or because of personality differences between men and women. However, clarifying the mentioned issues entails further researches in the future. On the basis of the results of this study, it is concluded that educating spouses about the patients’ needs is vital. In this way, it is suggested that the experiences of support of people with MS by their spouses be explored and the role of gender and level of education in relation to support be assessed in future studies. Hopefully, this study will draw attention to the paucity of good-quality evidence, improve the quality of future research, and highlight areas in which future studies could be directed usefully. We hope that these steps lead to improvement in supporting strategies by patients’ spouses with MS. This would result in alleviating problems, limitations, and stresses in their daily lives. In fact, we expect that the findings will give nurses and other healthcare experts a deeper perception of how to support people with MS and how to help and educate their spouses for supporting patients in coping with the disease. In addition, the findings can serve as a framework for developing nursing care processes, for planning educational sessions about physical and emotional support skills, and for establishing counseling and support programs, and patients’ ideological and cultural backgrounds would be considered as well.
Summary Statement
Why is this research or review needed?
- Previous studies have found that most informal caregivers who support people with MS were their spouses.
- Although people with MS are the main persons who experience support of their spouses, their understanding about spouses’ support has not yet been explored.
- Awareness of patients’ perception about spouses’ support and their needs and expectations would help healthcare providers, especially nurses who are key members of the care system, to develop educational programs to provide better support for patients.
What are the three key findings?
- First, based on the experiences of patients with MS, despite having physical disabilities, patients need emotional support more than physical support; however, patients were supported by their spouses more physically than emotionally.
- Second, understanding patient’s needs, defining new mutual roles, and adjusting expectations were the other main points of support, which were experienced by patients. In fact, it is vital to continue couple life despite having a chronic debilitating disease.
- On the basis of the experience of the participants, the second issue would not be achieved except through establishing a friendly and comfortable relationship.
- Third, participants did not consider their activities being done by their spouses as a supportive action, but they experienced their spouses’ attempt to maintain and enhance their independency in functioning as a positive supportive action.
How should the findings be used to influence policy/practice/research/education?
- The findings will give nurses and other healthcare experts a deeper perception of how to support people with MS and how to help and educate their spouses in supporting patients to adapt to the disease.
- The findings can serve to create a framework for developing nursing care processes to plan educational sessions about physical and emotional support skills for people with MS and their spouses.
- These findings can help nurses to establish counseling and support programs while regarding patients’ ideological and cultural background
Author Information
Somayeh Ghafari, RN BScN, is a PhD Graduate in Nursing, from the Department of Nursing, University of Social Welfare and Rehabilitation Sciences (USWR), Tehran, Iran.
Questions or comments about this article may be directed to Masoud Fallahi Khoshknab, RN BScN PhD, at [email protected]. He is an Associate Professor in the Department of Nursing, USWR, Tehran, Iran.
Kian Norouzi, RN BScN PhD, is an Associate Professor of Nursing, USWR, Tehran, Iran.
Eisa Mohamadi, RN BScN PhD, is an Associate Professor of Nursing, Department of Nursing, Tarbiat Modares University, Tehran, Iran.
This study was supported by a grant from USWR, Tehran, Iran. The authors declare no conflicts of interest.
Acknowledgments
We sincerely appreciate all participants who cooperated with us in doing this study. We thank the University of Social Welfare and Rehabilitation (USWR) and MS Society of Tehran and Isfahan (Iran) for their support.
References
Benedict R. H. B., Wahlig E. L., Topciu R. A., Englert J., Schwartz E., Chapman B., Weinstock-Guttman B., Duberstein R. P. (2009). Personality traits in women with multiple sclerosis: Discrepancy in patient/partner report and disease course. Journal of Psychosomatic Research, 66, 147–154.
Bisschop M. I., Kriegsman D. M. W., Beekman A. F., Deeg D. J. H. (2004). Chronic diseases and depression: the modifying role of psychosocial resources. Social Science and Medicine, 59, 721–733.
Buchanan R. J., Radin D., Chakravorty B. J. (2009). Informal care giving to more disabled people with multiple sclerosis. Disability and Rehabilitation, 3, 1244–1256.
Buchanan R. J., Radin D., Huang C. H. (2010). Burden among male caregivers assisting people with multiple sclerosis. Gender Medicine, 7 (6), 637–646.
Buchanan R. J., Radin D., Huang C. H., Zhu L. (2010). Caregiver perceptions associated with risk of nursing home admission for people with multiple sclerosis. Disability and Health Journal, 3, 117–124.
Dalkhmoosh M., Ahmadi M. (2013). Culture-specifics in Iranian values: A study in three samples of three generations. Developmental Psychology, 2013 (34), 107–115.
Dennison L., Moss-Morris R., Chalder T. (2009). A review of psychological correlates of adjustment in patients with multiple sclerosis. Clinical Psychology Review, 29, 141–153.
Dennison L., Moss-Morris R., Silberb E., Galeac I., Chalder T. (2010). Cognitive and behavioural correlates of different domains of psychological adjustment in early-stage multiple sclerosis. Journal of Psychosomatic Research, 69, 353–361.
Druley J. A., Townsend A. L. (1998). Self-esteem as a mediator between spousal support and depressive symptoms: A comparison of healthy individuals and individuals coping with arthritis. Health Psychology, 17 (3), 255–261.
Ehteshamzade P. (2009). Gender roles of women: Evolution of the role and mental health of family. Journal of Woman and Culture, 11 (44), 23–37.
Elo S., Kyngäs H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62, 107–115.
Etemadifar M., Sahraiyan M. A. (2012). Increasing of MS prevalence in Iran. Retrieved from www.iranms.ir
Finfgeld-Connett D. (2005). Clarification of social support. Journal of Nursing Scholarship, 37 (1), 4–9.
Fisher J. D., Nadler A., Whitcher-Alagna S. (1982). Recipient reactions to aid. Psychological Bulletin, 91 (1), 27–54.
Gbrich C. (2007). Qualitative data analysis: An introduction (1st ed.). London, UK: Sage.
Gingold J. (2011). Who gets MS? Retrieved from http://www.nationalmssociety.org
Gleason M. E. J., Iida M., Bolger N., Shrout P. E. (2003). Daily supportive equity in close relationships. Personality and Social Psychology Bulletin, 29 (8), 1036–1045.
Granheim U. H., Lundman B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24, 105–112.
Green J., Thorogood N. (2004). Qualitative methods for health research (1st ed.). London, UK: Sage.
Holloway I. (2005). Qualitative research in health care (1st ed.). Berkshire, UK: Open University Press.
Janssens A. C., Doorn P. A., Boer J. B., Meché F. G., Passchier J., Hintzen R. Q. (2003). Impact of recently diagnosed multiple sclerosis on quality of life, anxiety, depression and distress of patients and partners. Acta Neurologica Scandinavica, 108 (6), 389–395.
Kleiboer A. M., Kuijer R. G., Hox J. J., Jongend P. J. H., Frequine T. M. F. S., Bensing J. M. (2007). Daily negative interactions and mood among patients and partners dealing with multiple sclerosis (MS): The moderating effects of emotional support. Social Science and Medicine, 64, 389–400.
Kleiboer A. M., Kuijer R. G., Hox J. J., Schreurs K. M. G., Bensing J. M. (2006). Receiving and providing support in couples dealing with multiple sclerosis: A diary study using an equity perspective. Personal Relationships, 13 (4), 485–501.
Krokavcova M., Jitse P., Dijk V., Nagyova I., Rosenberger J., Gavelova M., Groothoff J. W. (2008). Social support as a predictor of perceived health status in patients with multiple sclerosis. Patient Education and Counseling, 73, 159–165.
McCabe M. P., Di Battista J. (2004). Role of health, relationships, work and coping on adjustment among people with multiple sclerosis: A longitudinal investigation. Psychology Health and Medicine, 9, 431–439.
McKeown P., Porter-Armstrong A., Baxter G. D. (2003). The needs and experiences of caregivers of individuals with multiple sclerosis: A systematic review. Clinical Rehabilitation, 17, 234–248.
Newsom J. T., Nishishiba M., Morgan D. L., Rook K. S. (2003). The relative importance of three domains of positive and negative social exchanges: A longitudinal model with comparable measures. Psychology and Aging, 18 (4), 746–754.
Nordgren L., Asp M., Fagerberg I. (2008). Support as experienced by men living with heart failure in middle age: A phenomenological study. International Journal of Nursing Studies, 45, 1344–1354.
Polit D., Beck T. (2008). Nursing research: Generating and assessing evidence for nursing practice (8th ed.). London, UK: Lippincott Williams & Wilkins.
Radford T. (2011). A guide for caregivers. Retrieved from http://www.nationalmssociety.org
Roessler R. T., Rumrill P. D., Fitzgerald S. M. (2004). Predictors of employment status for people with multiple sclerosis. Rehabilitation Counseling Bulletin, 47, 96–103.
Rudick R. A. (1998). A 29-year-old man with multiple sclerosis. Journal of the American Medical Association, 280, 1432–1439.
Rusbult C. E., Van Lange P. A. M. (2003). Interdependence, interaction and relationships. Annual Review of Psychology, 54, 351–375.
Sandelowski M. (2000). Focus on research methods: Whatever happened to qualitative description? Research in Nursing and Health, 23, 334–340.
Schwartz L. A., Kraft G. H. (1999). The role of spouse responses to disability and family environment in multiple sclerosis. American Journal of Physical Medicine and Rehabilitation, 78 (6), 525–532.
Segrin C., Badger T. A., Meek P., Lopez A. M., Bonham E., Sieger A. (2005). Dyadic interdependence on affect and quality-of-life trajectories among women with breast cancer and their partners. Journal of Social and Personal Relationships, 22 (5), 673–689.
Shamsaei F., Mohamad K., Kermanshahi S., Vanaki Z. (2012). Meaning of health from the perspective of family member caregiving to patients with bipolar disorder. Journal of Mazandaran University of Medical Sciences, 22 (6), 52–65.
Simon R. W., Nath L. E. (2004). Gender and emotion in the United States: Do men and women differ in self-reports of feelings and expressive behavior? American Journal of Sociology, 109 (5), 1137–1176.
Stambor Z. (2005). Women report greater moral traditionalism, social compassion than men. American Psychological Association, 36 (1), 15.
Strauss A., Corbin J. (1998). Basics of qualitative research: Techniques and procedures for developing grounded theory. Thousand Oaks: CA: Sage.
Taylor P., Morin R., Cohn D., Clark A., Wang W. (2008). A paradox in public attitudes. Men or women: Who’s the better leader? Media Inquiries Contact: Pew Research Center, 202, 419–4328. Retrieved from http://pewresearch.org
Thoits P. A. (1995). Stress, coping, and social support processes: Where are we? what next? Journal of Health and Social Behavior, 10, 53–79.
Thorne S. E., Paterson B. L. (2001). Health care professional support for self-care management in chronic illness: Insights from diabetes research, Patient Education and Counseling, 42, 81–90.
Thorne S., Paterson B., Acorn S., Canam C., Joachim G., Jillings C. (2002). Chronic illness experience: Insights from a qualitative meta-study. Quality Health Research, 12 (4), 437–452.
Tong A., Sainsbury P., Craig J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19, 349–357.
Williams P., Barclay L., Schmied V. (2004). Defining social support in context: A necessary step in improving research, intervention, and practice. Qualitative Health Research, 14 (7), 942–960.
Wright D. L., Aquilino W. S. (1998). Influence of emotional support exchange in marriage on caregiving wives’ burden and marital satisfaction. Family Relations: Interdisciplinary Journal of Applied Family Studies, 47 (2), 195–204.
Ybema J. F., Kuijer R. G., Hagedoorn M., Buunk B. P. (2002). Caregiver burnout among intimate partners of patients with a severe illness: An equity perspective. Personal Relationships, 9 (1), 73–88.


