Caregivers of Older Persons With Multiple Sclerosis: Determinants of Health-Related Quality of Life

Selected By
Colleen Harris, MN, NP, MSCN, MSCS
Why is this important to me?
As you become older, you may need some assistance from a caregiver in order to maintain your daily activities. Around 30% of people with MS require assistance, which is most often provided by the patient’s spouse.
Caring for someone with MS can be stressful for the caregiver and lead to weakened immune system, fatigue, eating disorders, weight loss, and physical inactivity. Caregivers may experience lower health-related quality of life (HRQOL) due to:
Problems the patient experiences such as disability, cognitive problems, and depression.
Problems the caregiver experiences such as caregiver burden (response to the physical, psychological, social, and financial stress that comes with caring for someone with a chronic illness); depression, lack of leisure activities, and social isolation; employment and income concerns; and health problems of their own. Stress is associated with caregiving and can lead to increased stress hormones, putting such caregivers at risk for high blood pressure, diabetes, and other health problems.
Little is known about factors that influence the HRQOL of caregivers of older people with MS. Caregivers of older people with MS may have needs that are different and in addition to the needs of caregivers of younger people with MS, and older caregivers may be undergoing physical or mental changes of their own.
Who will benefit from reading this study/article?
An important limitation of this study is that mostly male Caucasian caregivers answered the surveys, and the results may not be generally applicable to other groups.
Who did the authors study?
This study examined 102 pairs of patients with MS and their caregivers who were 60 years old or older. Of the 102 caregivers, 95% were Caucasian, two-thirds were men, and 81% were the spouse of the person with MS.
What is the objective of this study?
Results showed:
- The overall mental and physical HRQOL of these caregivers was about the same as non-caregivers of the same age.
- A significant negative effect was seen on mental health of the caregiver if he or she was caring for someone with MS who was depressed.
- Caregiver burden was mild or moderate. Older caregivers may have adapted over time to helping someone with MS. In addition, a positive attitude about providing care may lead to a positive assessment of burden. Alternatively, caregivers may tend to hide their burden so as to not seem disloyal to their spouse with MS.
- Factors that impacted the mental HRQOL of the caregiver were the patient’s depression, the caregiver’s perceived level of burden, and if the caregiver had heart disease. Surprisingly, mental health quality of life was positively impacted by an increased level of burden and caregiver heart disease.
- Factors that impacted the physical HRQOL of the caregiver were caregiver health problems such as diabetes or arthritis and having an annual income of less than $50,000.
- The patient’s level of disability did not predict HRQOL of the caregiver.
An important component of holistic care of someone with MS is addressing the physical and mental concerns of the patient’s caregiver. Nurses should develop and implement strategies to assess and address the important factors that contribute to HRQOL of older caregivers of people with MS. Future studies should determine what interventions and support will best help older caregivers of people with MS achieve an optimal HRQOL.
How did the authors study this issue?
The authors enrolled 102 pairs of patients with MS and their care partners who were an average age of 61 years old and who visited one of four MS centers on Long Island, NY.
Caregivers answered surveys that assessed:
- Physical, mental, and social health
- Caregiver burden
- Cognitive and neuropsychological problems
Patients with MS answered surveys that addressed:
- Cognitive problems
- Risk for neuropsychological impairment
- Disability
- Depression
| SHARE: | |||||
For more resources, visit:
Original Article
Caregivers of Older Persons With Multiple Sclerosis: Determinants of Health-Related Quality of Life
Journal of Neuroscience Nursing
Marijean Buhse, Carol Della Ratta, Janet Galiczewski, Patricia Eckardt
Multiple sclerosis (MS) is a chronic, progressive neurological disease usually diagnosed between the ages of 20 and 50 years. MS is estimated to affect over 2.5 million people worldwide with a prevalence of approximately 400,000 people in the United States (Finlayson, Van Denend, & Hudson, 2004; Giordano et al., 2012). Persons with MS commonly report both physical and psychological symptoms. The progressive nature of this illness often necessitates the need for a caregiver. Moreover, with expanded treatment regimens, persons with MS are living longer, thus extending the time caregivers are needed (Hurwitz, 2009).
MS causes demyelination of the central nervous system and may result in physical symptoms such as fatigue, pain, visual impairments, weakness, mobility impairments, and bladder and bowel dysfunction (Klewer, Pohlau, Nippert, Haas, & Kugler, 2001; Marrie et al., 2009, 2008). Psychologically, persons with MS may experience impaired cognition and depression and have less social interaction. Most persons with MS experience progression of the disease with some level of disability within 15 years of diagnosis (National Multiple Sclerosis Society, 2006). For many, the resulting physical and psychological impairments present significant challenges to daily life.
Challenges experienced by the persons with MS increase as they age (DiLorenzo, Halper, & Picone, 2004). Current studies report that life expectancy for persons with MS are approximately only 7Y10 years less than age-matched populations (Redelings, McCoy, & Sorvillo, 2006). A person diagnosed in their 20s may live with increasing disability of MS for 50 years and may need to rely on others as the disease progresses. As the level of disability progressively increases, such individuals may need assistance from a caregiver. Daily assistance with personal care may be necessary, and the role of caregiver may extend over many years. Approximately 30% of persons with MS need daily care, and most often, it is a spouse providing informal caregiving (Holland & Northrup, 2006).
An informal caregiver has been defined as a family member or other person who normally provides the daily care or supervision of a frail or disabled person (Kasle, 1995). Being a caregiver takes both a physical and emotional toll and is associated with high stress levels (Schulz & Sherwood, 2008). Increased stress, an altered immune system, fatigue, eating disturbances, weight loss, and physical inactivity are frequently associated with caregiving (Neri et al., 2012). The features of particular diseases are likely to determine the effect on the caregiver (Morley et al., 2012), and normal physical and mental decline of the older population may alter the ability to perform this demanding role (Neri et al., 2012). Challenges to those providing care to older persons with MS are twofold. Caring for older persons often requires meeting both their physical and mental needs over an extended period, and it is during this time in which older caregivers may experience their own physical and mental decline. Long-term caregiver exposure to suffering of a loved one may directly influence health-related quality of life (HRQOL) of caregivers (Monin & Schulz, 2009).
HRQOL has been explored in caregivers of younger persons with MS and older caregivers in other progressive neurological diseases (Alzheimer disease, Parkinson disease, etc.). However, there is limited research exploring QOL of caregivers attending to older persons with MS. Identification of factors that influence QOL is an initial step in determining appropriate interventions for caregivers. Caregivers to older persons with MS may have both additional and different needs than caregivers to younger persons with MS. The impact of these factors on such caregivers’ mental and physical QOL has not been fully explored. Caregivers to older persons with MS play a critical role in achieving high-quality care for the person with MS. Such caregivers may be older, experiencing their own physical or mental decline that may impact their ability to function in this role. This area warrants further attention of healthcare professionals who specialize in MS.
Background and Significance
The role of the primary caregiver of a person with MS may be demanding and negatively affect their HRQOL (Phillips & Humphreys, 2009). Moreover, patient’s and caregiver’s characteristics mutually interact to affect HRQOL (Alshubaili, Ohaeri, Awadalla, & Mabrouk, 2008). Specific factors that impact caregiver HRQOL are described below.
Patient Factors Affecting HRQOL
Impaired cognition is common in persons with MS and is associated with reduced HRQOL among caregivers (Figved, Myhr, Larsen, & Aarsland, 2007), and discrepant perceptions between persons with MS and their informal caregivers regarding the issue of impaired cognition often exist (Finlayson, Shevil, & Cho, 2009). Impaired cognition may affect memory and problemsolving ability and reduce awareness. Previous research has shown that, when discrepancies exist, caregiver distress increases (Finlayson et al., 2009). Furthermore, increase in caregiver distress negatively impacts caregivers’ HRQOL (Figved et al., 2007).
QOL of significant others caring for persons with MS is adversely influenced by the depressive symptoms of the person with MS (Rivera-Navarro et al., 2009). Significant others have reported that being a companion to a person with MS with depressive symptoms is burdensome (Giordano et al., 2012). HRQOL was reported to be significantly reduced in these caregivers especially if they were older and women. Furthermore, if the patient was depressed and more disabled, there was a negative effect on the HRQOL of their caregiver (Aishubaili, Ohaeri, Awadalla, & Mabrouk, 2008).
Caregivers of persons with MS have a lower HRQOL than the general population (Patti et al., 2007). Caregivers reported a lower HRQOL if the person with MS was depressed, and their HRQOL was predicted by the overall health of the person with MS. Caregivers were affected by the patient’s depression and had increased stress and distress levels (Lehan, Arango-Lasprilla, Macias, Aguayo, & Villasenor, 2012).
Caregiver Factors Affecting HRQOL
Caregiver burden is a multidimensional response to the physical, emotional, psychological, social, and financial stress associated with caring for another person (Buhse, 2008). It has been reported that caregivers of persons with MS had significantly more burden than noncaregivers (Gupta, Goren, Phillips, & Stewart, 2012). Caregiver burden has been shown to have a negative effect on caregiver HRQOL (Buhse, 2008). In addition, burden increases as the number of hours of caregiving increases. Major predictors of caregiver burden have been reported as caregiver depression and the disability level of the patient (Khan, Pallant, & Brand, 2007; Rivera-Navarro et al., 2009). Caregiver burden could be predicted by feelings of hopelessness, lack of leisure activities, and social isolation of the caregiver (Akkus, 2011). Furthermore, caregivers who are the patient’s partner may sometimes feel a heavy responsibility, and their involvement in providing care can have an enormous impact on their QOL (Rees, O’Boyle, & MacDonagh, 2001).
Financial issues related to caring for the patient with MS have been shown to cause a decrease in caregiver HRQOL across several studies. Akkus (2011) found a significant relationship between caregiver burden and their income, working status, and financial difficulties. Alshubaili et al. (2008) reported lower income because of caregiver unemployment, and less education was a significant factor for risk of decreased HRQOL in caregivers of persons with MS. Lower income of caregivers was shown to be negatively related to HRQOL, and less monthly income was associated with economic strain and depression (Hughes, Giobbie-Hurder, Weaver, Kubal, & Henderson, 1999).
Caregiver morbidity is another important factor impacting QOL. Gupta et al. (2012) found that caregivers of persons with MS were more likely to utilize healthcare resources and had lower physical and mental QOL than noncaregivers. Such caregivers tended to have more health provider and emergency department visits and more hospitalizations than noncaregivers. Specific health problems identified in caregivers of persons with MS were noted to include fatigue, back pain, anxiety, insomnia, shortness of breath, and depression (Forbes, While, & Mathes, 2007).
Stress associated with caregiving has been implicated in the development of caregiver morbidities (Vitaliano, Zhang, & Scanlan, 2003). Caregivers who were stressed were more likely to have higher levels of stress hormones compared with noncaregivers. This prolonged physiological reaction to elevated stress may put caregivers at a higher risk for hypertension, diabetes, and other comorbidities (Vitaliano et al., 2003). Family caregivers reported experiencing some kind of chronic illness and were taking psychopharmaceutical medication, receiving psychotherapeutic treatment, or both (Aymerich, Guillamon, & Jovell, 2009). These studies are limited in that the study samples were caregivers of younger persons with MS. Little is known about factors that impact caregivers of older persons with MS. The purpose of this study was to investigate factors associated with mental and physical HRQOL for persons caring for an older person with MS.
Theroetical Framework
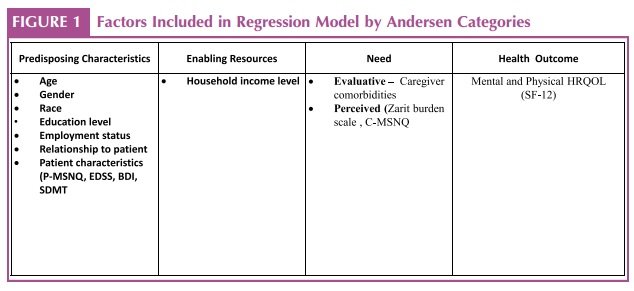
The Andersen (1995) Healthcare Utilization Model guided this study because it describes conditions that impact health status. The multitude of influences on health outcomes is represented in the model and may be of value in providing a comprehensive view of HRQOL in caregivers to older persons with MS. Knowledge of identified predictors of HRQOL may prompt nurses to address these areas at regular intervals to provide supportive care. In an adaptation of the Andersen Healthcare Utilization Model, health outcomes such as mental and physical HRQOL may occur as a result of the individual’s predisposing characteristics, enabling resources, and need (Andersen, 1995). These variables identified by the Andersen Model comprised the independent variables in this study and represent independent components that impact health status (Figure 1).
Predisposing characteristics, defined as demographics such as age or gender as well as education or employment, impact healthcare utilization. In this model, mutability, defined as that which can be easily changed, is an important concept. In this study, predisposing characteristics include caregiver age, gender, race, educational level, and employment status as well as their relationship to the patient. Because predisposing characteristics are viewed to have low mutability in this theoretical model, patient characteristics such as neuropsychiatric health, disability status, depressive symptoms, and cognition were included in this category. A second category described by Andersen (1995), enabling resources, represents those factors that impact use of healthcare services potentially impacting health status. Household income has been identified to represent enabling resources, impacting use and health outcomes. The third category, need for care, represents another important determinant of use of health services impacting health status. This includes biological need, termed level of disease. Level of disease has two components. Evaluative need is professional judgment about individual’s health status. Perceived need encompasses the individual’s view of their health status, experience of symptoms, and their perceptions of the magnitude and importance of their problems. In this study, need for care variables included the presence of caregiver comorbidity and their perception of health status. Comorbidities were determined to be present if the caregiver was currently taking prescribed medication for the health condition. Perceived health status included measures of burden and their perceptions of neuropsychiatric impairment of the person with MS for whom they care for.
According to Andersen (1995), individuals’ perceived needs may be altered through educational initiatives. Thus, the potential for advanced practice nurses to address QOL issues for caregivers to older patients with MS is vast. However, the first step is to fully understand the unique contribution of each predictor of HRQOL using a theoretically based multivariate approach. The identification of predictors that influence caregiver QOL is the initial step in determining appropriate interventions. Caregivers to older persons with MS may have additional and different needs than caregivers to younger persons with MS.
Method
A cross-sectional descriptive design was used to examine factors (patient and caregiver, clinical and demographic) to explain caregiver physical and mental HRQOL. Persons with MS aged 60 years or older and their caregivers from four MS centers on Long Island were included in the study. Caregivers of the persons with MS completed demographics, the Medical Outcomes Study Short Form 12 Health Survey (SF-12; HRQOL measure), Zarit Burden Interview, and the Caregiver MS Neuropsychological Screening Questionnaire (C-MSNQ). Persons with MS completed the Patient MS Neuropsychological Screening Questionnaire (P-MSNQ), oral Symbol Digit Modalities Test (SDMT, measure of cognitive function), Expanded Disability Status Scale (EDSS), and Beck Depression Inventory-2nd edition (BDI-II). All participants provided written informed consent at the time of recruitment. Institutional review board approval for this research was granted from the researchers’ university and the local institutional review board of MS Centers that participated in this study.
This study was part of a larger study on persons with MS over the age of 60 years; thus, inclusion criteria were patient age greater than 60 years and their informal caregivers. Both the patient and the caregiver had to have the ability to understand and sign consent and answer the surveys. If the patient was physically unable to complete the surveys themselves but were cognitively able, they were included in the study if they had someone who would write their answers for them. This ability was determined by the healthcare practitioner at each site. Exclusion criteria were severe cognitive impairment of the patient as determined by the healthcare practitioner at each site. Formal, paid caregivers were not included in this study. A self-selected, convenience sample of patients and caregivers who expressed an interest in participating were recruited into the study.
Sample
MS-caregiver dyads (n = 102) self-selected into the study. Healthcare practitioners in each center explained the research to age-appropriate patients and caregivers. Those who expressed an interest in participating were recruited into the study. At the time of recruitment, an oral SDMT was performed by all patient participants (Smith, 1968). Patient and caregiver participants were given the opportunity to complete the first survey during this healthcare visit.
Data Collection Procedure
Caregiver participants completed a demographic survey, the Zarit Burden Scale, the SF-12, and the C-MSNQ. MS participants were asked to complete the first of three different 15-minute cross-sectional paper-based surveys designed to identify issues that persons aged 60 years or older regularly face. If either participant chose to complete the first survey at another time, they were given a self-addressed postage paid envelope to mail it to the investigators. Upon return of this first survey, all participants were compensated a nominal amount for completing the questionnaires. Two other surveys were mailed to the patients’ home within a few weeks of their office visit; patients received a nominal amount for completing the surveys. With the objective of identifying issues that caregivers and patients face regularly, sociodemographic, clinical data and several validated scales were used to assess a series of health-related measures.
Measures
Caregiver Surveys
HRQOL of the caregiver was measured using the SF-12 (Ware, Kosinski, & Keller, 1996). The SF-12 is a short, generic measure of subjective health status. It contains 12 items from the original SF-36, which include the self-assessment of health, physical functioning, physical role limitation, mental role limitation, social functioning, mental health, and pain (Ware et al., 1996). The physical health and mental health summary scores have been shown to account for most of the variance in the eight subscales of health functioning and differentiate well between groups known to differ in the presence and seriousness of physical and mental conditions, acute symptoms, age and aging, self-reported changes in health, and recovery from depression.
Caregiver burden was measured using the Zarit Burden Interview (Zarit, Reever, & Bach-Peterson, 1980). This version contains 22 items in which each item on the interview is a statement that the caregiver is asked to endorse using a 5-point scale. Response options range from 0 (never) to 4 (nearly always). The Zarit Burden Interview assesses the level of burden experienced by the principal caregivers of older persons with senile dementia and persons with disability. It explores caregiver’s health, psychological well-being, finances, social life, and the relationship between the caregiver and the impaired person (Zarit et al., 1980).
Perceptions of cognitive and neuropsychological changes were measured using the Informant MS Neuropsychological Questionnaire and P-MSNQ (Benedict et al., 2003). This is a brief (10-minute) 15-item questionnaire assessing informant and patient perceptions of cognitive and neuropsychological changes in MS. Items used for screening impairments are scored on a 5 point scale (0Y4) accounting for both frequency and severity of symptoms. Informant reports are strongly correlated with the actual performance on cognitive testing of the person with MS (Benedict et al., 2004).
Patient Surveys
Cognitive function was measured using the oral SDMT (Smith, 1968). This was completed at the time of recruitment with the assistance of the healthcare provider. Respondents were provided with a worksheet containing rows of blank squares, each of which was associated with a symbol. The worksheet also contained a key matching each symbol with a corresponding number. Using the symbol key, respondents were given 90 seconds to verbalize as many numbers as possible. The more correct numbers verbalized, the higher the score, indicating better cognitive function (Smith, 1968).
Risk for neuropsychological impairment was measured using the P-MSNQ (Benedict et al., 2003). This scale consists of 15 items rated on a 5-point scale of 0 (never, does not occur) to 4 (very often, very disruptive), which are used to assess frequency and disruption levels of everyday life functioning, neuropsychological functioning, and mood in MS. The scores range from 0 to 60; higher scores indicate higher risk for neuropsychological impairment (Benedict et al., 2003).
Disability was measured using the self-reported version of the EDSS (Bowen, Gibbons, Gianas, & Kraft, 2001). This scale includes 19 self-rated items related to walking ability, strength, coordination, sensation, bladder, vision, swallowing, thinking, and MS disease activity. Scores range from 0 to 10, with higher scores indicating more advanced disease (Bowen et al., 2001).
The presence and severity of symptoms of depression were assessed using the BDI-II (Beck, Steer, & Brown, 1996). This 21-item instrument includes several symptoms of depression, which are rated on a 4-point scale ranging from 0 to 3 and has a maximum score of 63. Patients with a score of 0Y13 are considered to have minimal depression, 14Y19 are mild, 20Y28 are moderate, and 29Y63 are severe (Beck et al., 1996). Patients who scored greater than 28 were referred back to their healthcare provider.
Data Analysis
Data analysis was performed using Statistical Package for the Social Sciences software version 20.0. Descriptive statistics were computed on subjects’ demographic and clinical variables (health-related measures) to describe sample characteristics. Mean scores for caregivers’ physical and mental component summary of the SF-36 were compared with normative means. The modified Andersen Healthcare Utilization model domains and the current literature were used to select and categorize variables from the surveys for the multivariate regression models. These domains and the variables within each are displayed in Figure 1. This model provides a comprehensive view of the potential influences on caregiver HRQOL.
The relationship between patient and caregiver variables and the outcome variables (caregiver physical and mental HRQOL) was explored in separate analysis using Pearson correlations. The significant correlations were added to each regression model in order, starting from the highest correlation to develop two separate models for predicting caregiver mental and physical HRQOL. Multivariate linear regression was used to examine patient and caregiver variables to explain caregiver physical and mental HRQOL. The regression coefficients for each analysis represent the extent to which caregiver-QOL physical and mental scores (dependent variables) are expected to increase or decrease (if coefficient is negative) when specific factors (independent variables) are present, keeping other independent variables constant. Level of significance for all statistical tests was set at .05.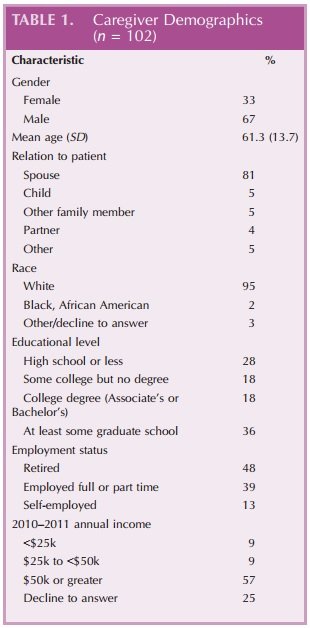
Results
Caregiver Demographic Characteristics
One hundred two patientYcaregiver dyads participated in the research. The self-reported demographics of the 102 caregiver sample revealed an almost entirely White race (95%), men comprising two thirds (66.7%) of the sample, and an average age of 61.83 (SD = 13.48) years. The caregivers in this study largely cohabitated with the person with MS (86%), and 81% of them were the spouse. Seventy-one percent of the sample had attended college or attained a college degree. Nearly half of the caregivers (48%) were currently retired. In the analysis of caregiver income, 25% declined to answer; those who did state income (n = 76), 75% were above $50,000 annual income (Table 1). The most common comorbidities of the caregiver respondents were arthritis and heart disease.
Health-Related Quality of Life
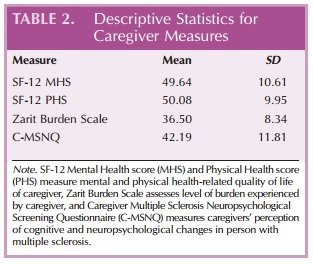
The caregivers in this sample reported overall mental HRQOL (M = 49.64, SD = 10.61) and physical HRQOL (M = 50.08, SD = 9.95) similar to population norms in their age group (49.87 for mental and physical). There was a statistically significant effect on mental QOL for caregivers caring for a person with MS who was depressed (as measured by the BDI-II). Lower mental HRQOL was found (t(41.62) = 3.11, p = .003) in this group. The caregivers in this group reported a mild-tomoderate burden score (M = 36.50, SD = 8.34) and perceived those they cared for to have neuropsychiatric impairment (M = 42.19, SD = 11.81).
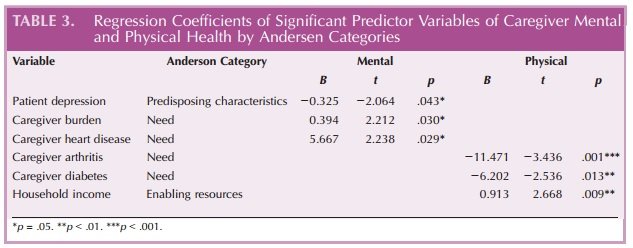
The mean P-MSNQ score among the patients was 28.35 (SD = 9.3) and was negatively correlated with the caregiver MSNQ (r = j.281, p = .005). Discrepancies between caregiver score and patient score indicated that the patient was at high risk for neuropsychological impairment. In addition, the scores on the SDMT indicated that the patients in this sample were cognitively impaired (M = 32.06). The patient disability score was 5.74 (SD = 1.84), which revealed that they could still ambulate about 300 feet without assistance, yet their activities of daily living were severely impacted. The mean score of the patients’ BDI-II was 11.48 (SD = 9.33) indicating that most patients were minimally depressed. The patient’s level of depression (BDI-II) was significantly associated with a decreased mental QOL (r = j.355, p = .001). Table 2 presents the mean scores of caregiver measures (SF-12 Mental Health score, SF-12 Physical Health score, Zarit Burden Scale, and C-MSNQ). The multiple regression model for this sample showed that 46% variance of caregiver mental HRQOL (asmeasured by the SF-12) was explained by patient depression (as measured by BDI), perceived level of caregiver burden (Zarit Burden Scale), and caregiver heart disease comorbidity (F = 7.18, p = .000). Caregiverpredicted mental QOL scores were decreased when caring for a person with MS who was depressed. Surprisingly, caregiver-predicted mental QOL scores were increased with their increased perceived level of burden (Zarit Burden Scale) and caregiver heart disease. Although level of physical disability (EDSS) for the person with MS was not a significant predictor of caregiver mental QOL, the value was approaching significance (p = .08; Table 2). In the second multiple regression model for this sample, 37% of the variance of caregiver physical HRQOL (as measured by the SF-12) was explained by the presence of caregiver comorbidities (arthritis and diabetes) and annual income ($0kY50k; F = 7.58, p G .000). Caregiver chronic obstructive pulmonary disease was approaching significance (p=.069; Table 3). Caregiver-predicted physical QOL scores were decreased when the caregiver had arthritis, diabetes, and annual income of $0kY50k.
Discussion
In this study, composed largely of older caregivers (mean age = 61 years), we sought to determine the degree to which patient and caregiver clinical and sociodemographic factors are associated with mental and physical QOL of those caring for an older person with MS. According to Andersen’s Healthcare Utilization Model, health outcomes such as mental and physical HRQOL are impacted by patient or caregiver predisposing characteristics, enabling resources, and need (Andersen, 1995). Although mean HRQOL scores of caregivers in this sample were similar to population norms for their age group, significant factors associated with HRQOL were found. The major findings in our study predicting caregiver HRQOL were patient depression, caregiver comorbidities, and lower financial income. These are discussed below as patient factors followed by caregiver factors.
Patient Factors Affecting Caregiver
QOL Our findings revealed that caregivers of older persons with MS had worsening HRQOL related to specific patient factors. This finding is not unique to caregivers of persons with MS because caregivers of older patients with other progressive neurological diseases have been found to have decreased HRQOL because of factors such as patient depression and disease progression (O’Connor & McCabe, 2011). Age of patient was not a related factor in this sample’s caregiver HRQOL. This finding is similar to other studies with caregivers of persons with MS in which patient age was not related to caregiver HRQOL or burden (Buchanan & Huang, 2011; Rivera-Navarro et al., 2009)
Caregivers in our study were slightly older than caregivers in an earlier study by Buchanan, Radin, Chakravorty, and Tyry (2009). However, in Buchanan et al.’s study, caregivers were described as caring for persons who had a more disabling course of the disease (mean age = 48 years), and more than 67% used a motorized scooter/wheelchair (Buchanan et al., 2009). In our study, most patients could ambulate with assistance despite other effects of the disease.
Unlike other studies of caregivers of persons with MS (Figved et al., 2007; Finlayson & Cho, 2008), our sample did not reveal an association between patients’ cognitive impairment and caregiver HRQOL. This was an unexpected finding because most of the previous studies show associations. One explanation for this finding could be the age of both the patient and the caregiver and the length of their relationship. Older caregivers may have reduced expectations of their relationships, which may buffer them from decreased QOL (Figved et al., 2007).
In this study, patient depression was a predictor of caregivers’ mental HRQOL. Similar to other studies of patients with progressive neurological disease, both patient and caregiver depression impacted caregiver HRQOL (O’Connor & McCabe, 2011). Giordano et al. (2102) found that significant others of depressed persons with MS had lower psychological well-being. Moreover, depression is a consistent predictor of QOL in both patients and caregivers of patients with a progressive neurological disease (Martinez-Martin, Rodriguez-Blazquez, & Forjaz, 2012).
Although increased patient disability did not predict for decreased caregiver HRQOL in this sample, it was approaching significance. The studies on the effect of physical disability in persons with MS on caregiver QOL are mixed. Increased physical disability in the person with MS has been shown to increase the emotional burden of the caregiver (Morales-Gonzales, Benito-Leon, Rivera-Navarro, Mitchell, & GEDMA Study Group, 2004). In contrast, another study found that disease characteristics including higher disability status in the persons with MS were unrelated to their caregiver’s well-being (Sherman et al., 2007). In both of these studies, mean age of the caregiver was between 48 and 50 years, and they were predominately women. The caregivers in our study were older (mean age = 61 years) and predominately men. It is possible that older persons with MS and their older caregivers have adapted to the physical changes over time, and for male caregivers, the role may not as physically demanding as it may be for women.
Caregiver Factors Affecting Caregiver QOL
Caregiver factors predicting poorer caregiver physical QOL included the presence of comorbidities and a lower financial income. Surprisingly, caregiver mental QOL was positively associated with caregiver burden. This is unusual because numerous studies of caregivers of persons with MS have shown that increased burden leads to decreased HRQOL (Buhse, 2008; Gupta et al., 2012; Khan et al., 2007; Rees et al., 2001).
Many caregivers deny the difficulties they face while giving care to their loved ones (Amendola, Oliveira, & Alvarenga, 2011). This may be because of feelings of self-acknowledgement for the role played; caregivers want to show that there are positive aspects attached to care. This role may give the caregiver positive feelings despite the burden of taking care of the patient and other daily life tasks. Positive feelings toward caregiving may contribute to a positive subjective assessment of burden. The older the person, the happier they rate their living situation despite negative factors affecting them (Blanchflower & Oswald, 2008). Many caregivers may be unwilling to reveal the true burden they are experiencing, perhaps for fear of seeming disloyal to their spouse (Rees et al., 2001).
Literature examining the effects of caregiver comorbidities is limited in caregivers of persons with not only MS but also all progressive neurologic diseases. As the population with MS ages, demands on formal caregivers will greatly increase, and this may negatively impact their physical health (Morley et al., 2012). As caregivers age, their own health-related issues and comorbidities may become a source of increased stress and decrease their overall QOL (DiLorenzo, 2011). Furthermore, caregivers of persons with MS have more activity impairment, more health provider office visits, more emergency department visits and more hospitalizations, and a lower mental and physical HRQOL than noncaregivers (Phillips, Stewart, Edwards, Gupta, & Goren, 2011).
In our study, caregiver physical HRQOL was negatively associated with caregiver arthritis and diabetes. This has been supported in previous studies examining comorbidities in caregivers of persons withMS. (Aymerich et al., 2009; Rivera-Navarro et al., 2009). Arthritis was the most frequent comorbidity affecting caregiver HRQOL in our study. This is not unexpected because arthritis is the most common cause of disability in older adults and steadily increases with age (Hootman, Helmick, & Brady, 2012). As the prevalence of arthritis increases, it often occurs with other chronic diseases, which may limit activity and thus HRQOL (Hootman et al., 2012). Caregivers with arthritis may find it more difficult to complete their own activities of daily living and limit their ability to care for the patient with MS.
Diabetes comorbidity was also found to be negatively associated with caregiver physical QOL. Diabetes is a common disease in aging people affecting approximately 26.9% of Americans over the age of 65 years (Centers for Disease Control and Prevention, 2011). Aging is a risk factor for diabetes and has been linked to higher mortality and reduced functional status. Older adults with diabetes are also at a substantial risk for cardiovascular disease (Kirkman et al., 2012). Older adults with diabetes reported nearly twice as many unhealthy days (physical or mental) than those adults without the disease (Brown et al., 2004). Furthermore, diabetes is independently associated with lower levels of HRQOL among older adults. Our study supports these findings. Lower caregiver HRQOL or reports of unhealthy days may impact the care provided to the older person with MS.
An unexpected finding in our study was that caregiver comorbidity of heart disease was positively correlated with mental HRQOL suggesting that caregivers with heart disease in this study had higher mental HRQOL. This is incongruent with findings in other populations of caregivers (Kim, Carver, Cannady, & Shaffer, 2013; Pinquart & Sorensen, 2003). This finding may be the result of self-reported data collection strategy used in this study. Caregivers were determined to have heart disease if they reported taking medications for this condition. This strategy may have overlooked those caregivers who may have a comorbidity but do not take medication. Moreover, there can be a lack of knowledge in patients as to what medications they take and for what disease (Nair et al., 2002).
Decreased financial income was a factor associated with lower caregiver physical HRQOL in our study. The financial losses experienced by families of persons withMS had a negative impact on their well-being (DeJubicibus & McCabe, 2005). Financial limitations impacted the QOL of families of those with MS by restricting their ability to engage in pleasurable activities and social interactions. In other diseases, such as cancer and Parkinson disease, lower financial income has also been shown to negatively affect the QOL of the patient and their families (Rees et al., 2001; Short, Vasey, & Tunceli, 2005).
Limitations
This study has limitations. Generalizability is limited to Caucasian, predominately male caregivers. In addition, most data in this study were self-reported, threatening the validity and accuracy of these reports. It is possible that the respondents have not accurately reported the retrospective data, may not wish to share their personal information, or aim to present themselves in a positive light. Despite these challenges, the selfreported data have yielded information that would otherwise be likely unobtainable. Another limitation was noted with respect to the presence of caregiver comorbidity. These were determined to be present if the caregiver acknowledged taking medication for a condition. This method excluded comorbidities that were undiagnosed or undertreated but still may have an effect on the caregivers’ HRQOL. Despite these limitations, these results, revealed in a study based on a theoretical framework, provide guidance for future research examining the needs of caregivers to older persons with MS.
Summary
The number of older persons living with MS is increasing as Baby Boomers age. Many of these older persons with MS are living longer despite physical and mental disabilities. This study has shown that these caregivers are generally the spouses of the persons with MS. For these older caregivers, ‘‘informal care’’ may be substantial in scope, intensity, and duration, which are often concomitant with their own physical, emotional, and financial limitations. This descriptive study, based on the Anderson Theoretical Model, provides insight into factors impacting older caregivers’ HRQOL. In this sample, patient depression, caregiver comorbidity, and decreased financial income negatively impacted the HRQOL of older caregivers.
Addressing mental and physical needs of these caregivers is an important component of holistic MS care and represents the essence of nursing. The role of the caregiver to an older person with MS may be viewed by the clinician as the linchpin to high-quality patientcentered care. Nurses who care for older persons with MS will increasingly rely on older caregivers to provide patient-centered interventions. Therefore, it is essential for nurses to develop and implement assessment protocols for those caregivers at risk for decreased HRQOL. Furthermore, it is the nurse’s role to develop strategies to reduce the impact of these factors to further assist older persons in their caregiving to older persons with MS. More research is necessary to elucidate the types of interventions that support these caregivers as they care for older persons with MS.
References
Akkus, Y. (2011). Multiple sclerosis patient caregivers: The relationship between their psychological and social needs and burden levels. Disability and Rehabilitation, 33(4), 326Y333. doi:10.3109/09638288.2010.490866
Alshubaili, A. F., Ohaeri, J. U., Awadalla, A. W., & Mabrouk, A. A. (2008). Family caregiver quality of life in multiple sclerosis among Kuwaitis: A controlled study. BMC Health Services Research, 8, 206. doi:10.1186/1472-6963-8-206
Amendola, F., Oliveira, M. A., & Alvarenga, M. R. (2011). Influence of social support on the quality of life of family caregivers while caring for people with dependence. Revista da Escola de Enfermagem da USP, 45(4), 884Y889.
Andersen, R. M. (1995). Revisiting the behavioral model and access to medical care: Does it matter? Journal of Health and Social Behavior, 36(1), 1Y10.
Aymerich, M., Guillamon, I., & Jovell, A. J. (2009). Health-related quality of life assessment in people with multiple sclerosis and their family caregivers. A multicenter study in Catalonia (Southern Europe). Journal of Patient Preference and Adherence, 3, 311Y321.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory-II manual San Antonio, TX: Psychological Corporation.
Benedict, R. H., Cox, D., Thompson, L. L., Foley, F., Weinstock-Guttman, B., & Munschauer, F. (2004). Reliable screening for neuropsychological impairment in multiple sclerosis. Multiple Sclerosis, 10(6), 675Y678.
Benedict, R. H., Munschauer, F., Linn, R., Miller, C., Murphy, E., Foley, F., & Jacobs, L. (2003). Screening for multiple sclerosis cognitive impairment using a self-administered 15-item questionnaire. Multiple Sclerosis, 9(1), 95Y101.
Blanchflower, D. G., & Oswald, A. J. (2008). Is well-being U-shaped over the life cycle? Social Science and Medicine, 66(8), 1733Y1749. doi:10.1016/j.socscimed.2008.01.030
Bowen, J., Gibbons, L., Gianas, A., & Kraft, G. H. (2001). Selfadministered Expanded Disability Status Scale with functional system scores correlates well with a physician-administered test. Multiple Sclerosis, 7(3), 201Y206
Brown, D. W., Balluz, L. S., Giles, W. H., Beckles, G. L., Moriarty, D. G., Ford, E. S., & Mokdad, A. H.; Behavioral Risk Factor Surveillance System. (2004). Diabetes mellitus and health-related quality of life among older adults. Findings from the behavioral risk factor surveillance system (BRFSS). Diabetes Research and Clinical Practice, 65(2), 105Y115. doi:10 .1016/j.diabres.2003.11.014
Buchanan, R., & Huang, C. (2011). Health-related quality of life among informal caregivers assisting people with multiple sclerosis. Disability and Rehabilitation, 33(2), 113Y121. doi:10 .3109/09638288.2010.486467
Buchanan, R. J., Radin, D., Chakravorty, B. J., & Tyry, T. (2009). Informal care giving to more disabled people with multiple sclerosis. Disability and Rehabilitation, 31(15), 1244Y1256.
Buhse, M. (2008). Assessment of caregiver burden in families of persons with multiple sclerosis. Journal of Neuroscience Nursing, 40(1), 25Y31.
Centers for Disease Control and Prevention. (2011). National diabetes fact sheet: National estimates and general inforamtion on diabetes and prediabetes in the United States. Atlanta, GA: Author.
DeJubicibus, M.A., & McCabe, M. (2005). Economic deprivation and it’s effectson subjective well being in families of people with multiple sclerosis. Journal of Mental Health, 14, 49Y59.
DiLorenzo, T. (2011). Aging with multiple sclerosis: A clinical bulletin from the Professional Resource Center of the National Multiple Sclerosis Society. New York, NY: National Multiple Sclerosis Society
DiLorenzo, T., Halper, J., & Picone, M. (2004). Comparison of older and younger individuals with multiple sclerosis: A preliminary investigation. Rehabilitation Psychology, 49(2), 123Y125.
Figved, N., Myhr, K. M., Larsen, J. P., & Aarsland, D. (2007). Caregiver burden in multiple sclerosis: The impact of neuropsychiatric symptoms. Journal of Neurology, Neurosurgery, and Psychiatry, 78(10), 1097Y1102. doi:10.1136/jnnp.2006 .104216
Finlayson, M., & Cho, C. (2008). A descriptive profile of caregivers of older adults with MS and the assistance they provide. Disability and Rehabilitation, 30(24), 1848Y1857. doi:10 .1080/09638280701707324
Finlayson, M., Shevil, E., & Cho, C. C. (2009). Perceptions of cognitive symptoms among people aging with multiple sclerosis and their caregivers. American Journal of Occupational Therapy, 63(2), 151Y159.
Finlayson, M., Van Denend, T., & Hudson, E. (2004). Aging with multiple sclerosis. Journal of Neuroscience Nursing, 36(5), 245Y251, 259.
Forbes, A., While, A., & Mathes, L. (2007). Informal carer activities, carer burden and health status in multiple sclerosis. Clinical Rehabilitation, 21(6), 563Y575. doi:10.1177/0269215507075035
Giordano, A., Ferrari, G., Radice, D., Randi, G., Bisanti, L., Solari, A. & Posmos Study. (2012). Health-related quality of life and depressive symptoms in significant others of people with multiple sclerosis: A community study. European Journal of Neurology, 19(6), 847Y854. doi:10.1111/j.1468-1331.2011.03638.x
Gupta, S., Goren, A., Phillips, A., & Stewart, M. (2012). Selfreported burden among caregivers of patients with multiple sclerosis. International Journal of MS Care, 14, 179Y187.
Holland, N., & Northrup, D. (2006). Young adults with multiple sclerosis: Management in the home. Home Health Care Management and Practice, 18(3), 186Y195.
Hootman, J. M., Helmick, C. G., & Brady, T. J. (2012). A public health approach to addressing arthritis in older adults: The most common cause of disability. American Journal of Public Health, 102(3), 426Y433. doi:10.2105/AJPH.2011.300423
Hughes, S. L., Giobbie-Hurder, A., Weaver, F. M., Kubal, J. D., & Henderson, W. (1999). Relationship between caregiver burden and health-related quality of life. Gerontologist, 39(5), 534Y545.
Hurwitz, B. J. (2009). The diagnosis of multiple sclerosis and the clinical subtypes. Annals of Indian Academy of Neurology, 12(4), 226Y230. doi:10.4103/0972-2327.58276
Kasle, A. (1995). New York State elder law handbook. New York, NY: Sadin Institute on Law & Public Policy of the Brookdale Center for Healthy Aging and Longevity, Hunter College.
Khan, F., Pallant, J., & Brand, C. (2007). Caregiver strain and factors associated with caregiver self-efficacy and quality of life in a community cohort with multiple sclerosis. Disability and Rehabilitation, 29(16), 1241Y1250. doi:10.1080/ 01443610600964141
Kim, Y., Carver, C. S., Cannady, R. S., & Shaffer, K. M. (2013). Self-reported medical morbidity among informal caregivers of chronic illness: The case of cancer. Quality of Life Research, 22(6), 1265Y1272. doi:10.1007/s11136-012-0255-y
Kirkman, M. S., Briscoe, V. J., Clark, N., Florez, H., Haas, L. B., Halter, J. B., I Swift, C. S. (2012). Diabetes in older adults. Diabetes Care, 35(12), 2650Y2664. doi:10.2337/dc12-1801
Klewer, J., Pohlau, D., Nippert, I., Haas, J., & Kugler, J. (2001). Problems reported by elderly patients with multiple sclerosis. Journal of Neuroscience Nursing, 33(3), 167Y171.
Lehan, T., Arango-Lasprilla, J. C., Macias, M. A., Aguayo, A., & Villasenor, T. (2012). Distress associated with patients’ symptoms and depression in a sample of Mexican caregivers of individuals with MS. Rehabilitation Psychology, 57(4), 301Y307. doi:10.1037/a0030764
Marrie, R., Horwitz, R., Cutter, G., Tyry, T., Campagnolo, D., & Vollmer, T. (2008). Comorbidity, socioeconomic status and multiple sclerosis. Multiple Sclerosis, 14(8), 1091Y1098. doi:10.1177/1352458508092263
Marrie, R. A., Horwitz, R., Cutter, G., Tyry, T., Campagnolo, D., & Vollmer, T. (2009). The burden of mental comorbidity in multiple sclerosis: Frequent, underdiagnosed, and undertreated. Multiple Sclerosis, 15(3), 385Y392. doi:10.1177/ 1352458508099477
Martinez-Martin, P., Rodriguez-Blazquez, C., & Forjaz, M. J. (2012). Quality of life and burden in caregivers for patients with Parkinson’s disease: Concepts, assessment and related factors. Expert Review of Pharmacoeconomics & Outcomes Research, 12(2), 221Y230. doi:10.1586/erp.11.106
Monin, J. K., & Schulz, R. (2009). Interpersonal effects of suffering in older adult caregiving relationships. Psychology and Aging, 24(3), 681Y695. doi:10.1037/a0016355
Morales-Gonzales, J. M., Benito-Leon, J., Rivera-Navarro, J., Mitchell, A. J., & GEDMA Study Group. (2004). A systematic approach to analyse health-related quality of life in multiple sclerosis: The GEDMA study. Multiple Sclerosis, 10(1), 47Y54.
Morley, D., Dummett, S., Peters, M., Kelly, L., Hewitson, P., Dawson, J., I Jenkinson, C. (2012). Factors influencing quality of life in caregivers of people with Parkinson’s disease and implications for clinical guidelines. Parkinson’s Disease, 2012, 190901. doi:10.1155/2012/190901
Nair, K., Dolovich, L., Cassels, A., McCormack, J., Levine, M., Gray, J., I Burns, S. (2002). What patients want to know about their medications. Focus group study of patient and clinician perspectives. Canadian Family Physician, 48, 104Y110.
National Multiple Sclerosis Society. (2006). What Is MS? Retrieved from http://www.nationalmssociety.org/What-is-MS
Neri, A. L., Yassuda, M. S., Fortes-Burgos, A. C., Mantovani, E. P., Arbex, F. S., de Souza Torres, S. V., I Guariento, M. E. (2012). Relationships between gender, age, family conditions, physical and mental health, and social isolation of elderly caregivers. International Psychogeriatrics, 24(3), 472Y483. doi:10 .1017/S1041610211001700
O’Connor, E. J., & McCabe, M. P. (2011). Predictors of quality of life in carers for people with a progressive neurological illness: A longitudinal study. Quality of Life Research, 20(5), 703Y711. doi:10.1007/s11136-010-9804-4
Patti, F., Amato, M. P., Battaglia, M. A., Pitaro, M., Russo, P., Solaro, C., & Trojano, M. (2007). Caregiver quality of life in multiple sclerosis: A multicentre Italian study. Multiple Sclerosis, 13(3), 412Y419. doi:10.1177/1352458506070707
Phillips, A. L., Stewart, M., Edwards, N., Gupta, S., & Goren, A. (2011). The hidden toll of caregiver burden in multiple sclerosis. Paper presented at the 18th Annual Meeting of the International Society for Pharmacoeconomics and Outcomes Research, Baltimore, MD, USA
Phillips, C. J., & Humphreys, I. (2009). Assessing cost-effectiveness in the management of multiple sclerosis. ClinicoEconomics and Outcomes Research, 1, 61Y78.
Pinquart, M., & Sorensen, S. (2003). Differences between caregivers and noncaregivers in psychological health and physical health: A meta-analysis. Psychology and Aging, 18(2), 250Y267.
Redelings, M. D., McCoy, L., & Sorvillo, F. (2006). Multiple sclerosis mortality and patterns of comorbidity in the United States from 1990 to 2001. Neuroepidemiology, 26(2), 102Y107. doi:10.1159/000090444
Rees, J., O’Boyle, C., & MacDonagh, R. (2001). Quality of life: Impact of chronic illness on the partner. Journal of the Royal Society of Medicine, 94(11), 563Y566.
Rivera-Navarro, J., Benito-Leon, J., Oreja-Guevara, C., Pardo, J., Dib, W. B., Orts, E., & BellF, M.; Caregiver Quality of Life in Multiple Sclerosis Study Group. (2009). Burden and healthrelated quality of life of Spanish caregivers of persons with multiple sclerosis. Multiple Sclerosis, 15(11), 1347Y1355. doi:10.1177/1352458509345917
Schulz, R., & Sherwood, P. R. (2008). Physical and mental health effects of family caregiving. The American Journal of Nursing, 108(9 Suppl.), 23Y27. doi:10.1097/01.NAJ.0000336406 .45248.4c
Sherman, T. E., Rapport, L. J., Hanks, R. A., Ryan, K. A., Keenan, P. A., Khan, O., & Lisak, R. P. (2007). Predictors of well-being among significant others of persons with multiple sclerosis. Multiple Sclerosis, 13(2), 238Y249. doi:10.1177/ 1352458506070754
Short, P. F., Vasey, J. J., & Tunceli, K. (2005). Employment pathways in a large cohort of adult cancer survivors. Cancer, 103(6), 1292Y1301. doi:10.1002/cncr.20912
Smith, A. (1968). The symbol digit modalities test: A neuropsychologic test of learning and other cerebral disorders. Seattle, WA: Special Child Publications.
Vitaliano, P. P., Zhang, J., & Scanlan, J. M. (2003). Is caregiving hazardous to one’s physical health? A meta-analysis. Psychological Bulletin, 129(6), 946Y972. doi:10.1037/0033-2909 .129.6.946
Ware, J. Jr., Kosinski, M., & Keller, S. D. (1996). A 12-item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220Y233.
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist, 20(6), 649Y655.

