Multiple Sclerosis and Sexuality

Selected By
June Halper, MSN, APN-C, MSCN, FAAN
Why is this important to me?
MS affects many aspects of a person’s life, including sexuality. Around 80% of people with MS report sexual problems, which may be due to muscle weakening, bladder and/or bowel problems, abnormal sensation, especially in the genital regions, and psychological factors.
Who will benefit from reading this study/article?
People with MS who are or may become involved in a sexual relationship in the future will benefit from reading this article.
What is the objective of this study?
In general, sexual problems in MS may be due to neurological changes as a direct result of the disease, MS-related changes in areas that indirectly affect sexual function such as fatigue and bladder and bowel problems, and psychological effects such as body image and mood. Women with MS sometimes have problems with genital sensation, decreased vaginal lubrication, problems achieving orgasm, and decreased desire. Men with MS may have problems with erections and ejaculation. The author identified several MS symptoms that may lead to sexual problems:
- Fatigue: Up to 95% of people with MS experience fatigue, which may be due to muscle spasticity and exhaustion from performing daily activities. If you are tired at the end of the day, you may not have enough energy for sexual activity. Physiotherapy or occupational therapy may provide strategies for conserving energy, which may increase your interest in sex. Alternative sex positions and alternatives to intercourse may use less energy and increase satisfaction.
- Bladder and bowel dysfunction: Embarrassment as well as incontinence or the fear of incontinence may lessen interest in sex. Emptying your bladder before sex may help with incontinence. Also be aware that sex is possible even if you have a catheter.
- Muscle spasms: Muscle spasms can occur without warning and may be painful, which may decrease your interest in sex. Some medications can help, but may have sedative-like side effects.
- Nerve pain: Nerve pain can occur anywhere in the body and may lessen your interest in sex, especially when the pain is in your genital area. Nonmedical treatments such as massage, acupuncture, and hot and cold packs may help.
- Depression: Around 50% of people with MS experience depression. Medications that treat depression may cause or worsen sexual problems.
- Body image problems: Mobility problems and other disabilities affect your physical body and may make you feel unattractive or undesirable. Such issues, even if you are in a stable, long-term relationship, may cause you and your partner stress.
A healthy, satisfying sex life is possible, even with a chronic disease such as MS. If you are comfortable doing so, talk to a trusted nurse who is trained in methods to help you talk about and overcome sexual difficulties.
How did the author study this issue?
The author reviewed symptoms of MS that may influence sexual dysfunction and offered some possible solutions.
Original Article
Multiple Sclerosis and Sexuality
American Journal of Nursing
Anne Katz, PhD, RN
Multiple sclerosis (MS) is a progressive disease affecting the central nervous system. There are currently four recognized subtypes of the disease, defined according to the frequency and severity of symptoms; MS can have a relapsing-remitting course, with exacerbations followed by periods of remission, or it can progress without remission, although relapsing types usually cause more damage and remission periods shorten over time. MS most commonly appears between the ages of 20 and 50 years. Although some people have relatively few problems, others will be severely affected; disease progression can be rapid or more indolent. All aspects of daily life may be affected, including sexual functioning, which may be altered as a result of hanges in muscle strength; problems with bladder and bowel functioning; and altered sensation, particularly in the genital region. 
HOW IS SEXUALITY AFFECTED?
A 2006 study by Demirkiran and colleagues showed that more than 80% of patients with MS experienced sexual dysfunction. Foley and colleagues developed a conceptual model of sexual difficulties in people with MS that comprises three levels. In this model, primary sexual dysfunction occurs as a result of neurologic changes directly affecting sexual response or feelings (or both). According to a study by McCabe and colleagues, women most commonly describe altered genital sensations, diminished vaginal lubrication, difficulty achieving orgasm, and a loss of desire. Men experience difficulty achieving and maintaining erections as well as ejaculatory problems (failing or taking too long to ejaculate; the rate of premature ejaculation in the study wasn't statistically different from that in the general population). Secondary sexual dysfunction is caused by MS-related physical changes that don't directly affect sexual functioning through nervous system pathways. Examples of these are fatigue and bladder and bowel problems. Tertiary sexual dysfunction refers to the psychosocial aspects of the disorder that can significantly affect sexual functioning, such as body image, mood, and sexual self-image. Dysfunction at any of these three levels can be distressing to a patient, however, and several of these are worth noting.
SEXUAL CHALLENGES IN MS
Fatigue is experienced by as many as 95% of patients with MS and can have several causes. Energy is used in coping with activities of daily living and with temperature changes in the environment, particularly heat, which are often taxing to patients with MS. Muscle spasticity (involuntary muscle stiffness) also consumes energy, and people with symptomatic MS are usually very tired at the end of the day. This can mean that they lack sufficient energy for sexual activity. The nurse working with such a patient may want to make some suggestions for conserving energy or dealing more effectively with the lack of energy. A referral to physiotherapy or occupational therapy may be in order; such therapists can provide strategies for energy conservation during daily activities, which may stimulate greater interest in sexual activity. Patients with MS may be able to identify the times of day when they have the most energy (perhaps after a nap or early in the morning) in order to engage in sexual activity. The use of stimulants such as caffeine can be counterproductive because they can cause bladder irritation, bladder spasms, or incontinence. Alternative positioning for sexual intercourse may be helpful, too; the side-lying and bottom positions use less energy. Alternatives to intercourse (such as oral sex) may also use less energy and provide satisfaction for both parties.
Bladder and bowel concerns. One possible challenge during sexual activity for the person with MS is incontinence, either urinary or fecal. Even if it has never occurred, the patient's fear may be so great that she or he avoids sexual activity altogether-"just in case." If the person with MS cannot empty her or his bladder completely, there may be pressure in the pelvic area that interferes with sexual pleasure. Emptying the bladder completely just before sexual activity can help with this. Restricting fluid intake and avoiding diuretic beverages such as coffee and diet soda may also help.
Passing flatus or leaking feces during sexual activity can be very embarrassing. In addition, constipation can make intercourse uncomfortable. Careful use of laxatives and stool softeners may help, although it's important to avoid diarrhea, which may itself cause fecal incontinence. Some people with MS may need manual extraction to empty the rectum of feces.
Catheters. Some people with MS have an indwelling catheter, which might appear to completely preclude sexual activity, but for the motivated couple sexual intercourse is possible; women should bring the catheter forward (away from the vaginal introitus) and tape it securely to the leg; men can bring it backward along the length of the penis and anchor it in place with a condom. Friction may cause irritation to the urethra for both men and women so stabilizing the catheter is important.
Muscle spasm and spasticity. Some people with MS experience muscle spasms or spasticity (or both), which can directly affect their ability to participate in pleasurable sexual activity. Muscle spasms usually occur without any warning, and the pain will definitely interfere with any pleasurable activity. Spasticity may interfere with comfortable positioning. Medications such as muscle relaxants and antiseizure agents can treat both of these symptoms, but they're often sedating. Taking medication about 20 minutes before sexual activity may be helpful. Experimenting with different positions can also help the couple find a way to be sexual without causing pain or discomfort, but it takes a motivated couple to do this.
Nerve or neuropathic pain occurring anywhere in the body-but particularly in the genital area-is another challenge to a satisfying sexual life. Treating nerve pain can be challenging, too, and many of the medications used to treat it have significant adverse effects. However, nonmedical interventions, such as massage therapy, acupuncture, and biofeedback, can help and have no significant adverse effects. Some people also report that the application of hot and cold packs to the area three times a day can help alleviate pain.
Depression. As many as 50% of patients with MS have experienced at least one major episode of depression. It may be physiologic in nature and caused by brain lesions or a reaction to the challenges of living with MS and the many losses experienced as part of the disease process. Although pharmacologic treatment for depression is highly effective, many of the newer selective serotonin reuptake inhibitors (SSRIs) have significant sexual adverse effects, including difficulty achieving orgasm or arousal. Such medications may further exacerbate sexual problems caused by MS itself or create new ones.
Body image difficulties. MS causes changes to the physical body resulting from muscle wasting, weight gain (a consequence of inactivity), and mobility issues. For many with this disease, this can cause a negative body image. Not everyone experiences this, but some patients may feel unattractive and undesirable, further challenging any hope of an active and satisfying sex life. Body image issues can affect even long-term relationships and can cause significant distress to both the person with MS and the partner.
DISCUSSING MS WITH PATIENTS
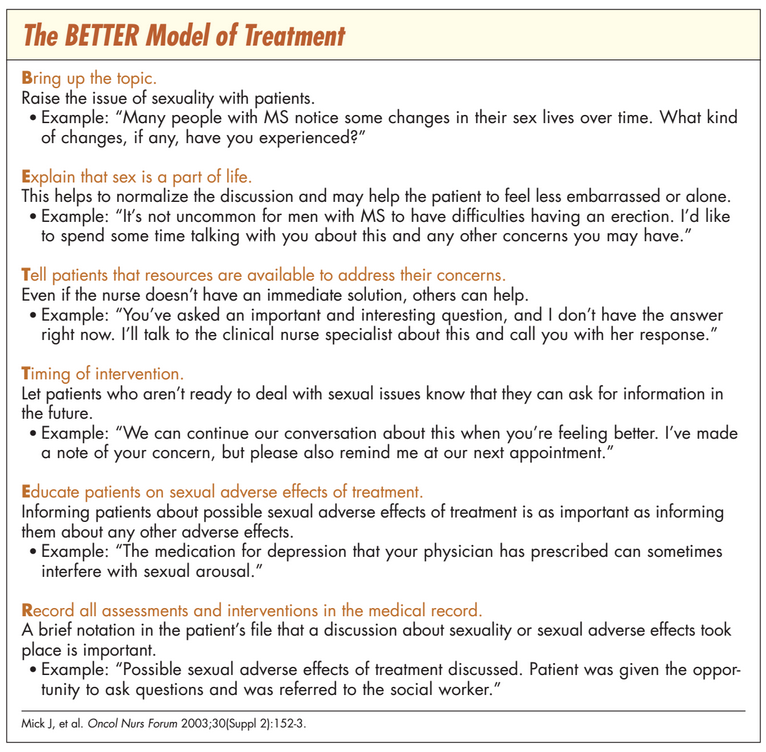
The first step for the patient with MS who's experiencing sexual difficulties is to talk about it. Many people assume that a healthy and satisfying sex life isn't possible in the context of a chronic disease like MS, but that simply isn't true. Nurses are in the perfect position to provide education to patients regarding the realities of living with MS, as well as adapting and adjusting to the many associated challenges. For help in starting conversations about sexuality and MS, see The PLISSIT Model of Treatment and The BETTER Model of Treatment.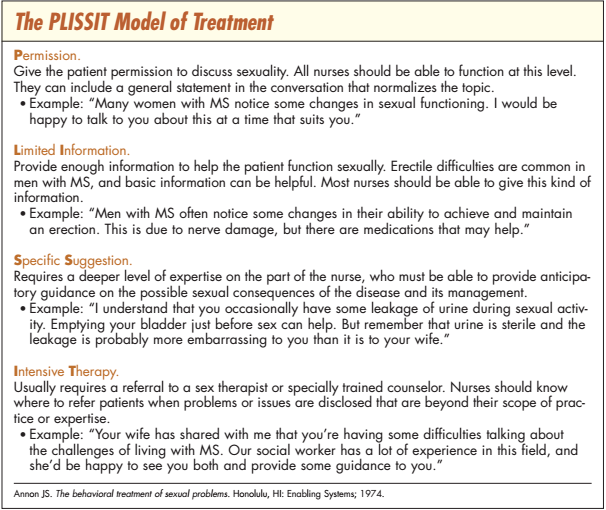
Specific interventions are limited. Research has shown that some men with MS find sildenafil (Viagra) to be helpful with erectile difficulties. There are no medications approved for arousal problems in women. Vaginal moisturizers, such as Replens, may be helpful for women experiencing vaginal dryness; lubricants, especially silicone-based products, can be helpful when dryness interferes with penetrative intercourse.
In short, the nurse should remember that MS remains a disease with many serious effects on the quality of patients' lives. Nurses will interact with these patients in many different areas of both hospital and ambulatory care, which provides ample opportunity to ask them about their sexuality and provide support and possibly assistance with problems they experience.
REFERENCES
1. McCabe MP. Relationship functioning and sexuality among people with multiple sclerosis. J Sex Res 2002;39(4):302-9.
2. Moore LA. Intimacy and multiple sclerosis. Nurs Clin North Am 2007;42(4):605-19; vii.
3. Schmidt EZ, et al. Sexuality in multiple sclerosis. J Neural Transm 2005;112(9):1201-11.
4. Demirkiran M, et al. Multiple sclerosis patients with and without sexual dysfunction: are there any differences? Mult Scler 2006;12(2):209-14.
5. Foley FW, et al. Rehabilitation of intimacy and sexual dysfunction in couples with multiple sclerosis. Mult Scler 2001;7(6):417-21.
6. Gagliardi BA. The experience of sexuality for individuals living with multiple sclerosis. J Clin Nurs 2003;12(4):571-8.
7. Hutchinson J. Multiple sclerosis, body image and sexuality. Nurs Times 2006;102(19):50-5.
8. Fowler CJ, et al. A double blind, randomised study of sildenafil citrate for erectile dysfunction in men with multiple sclerosis. J Neurol Neurosurg Psychiatry 2005;76(5):700-5.
9. Safarinejad MR. Evaluation of the safety and efficacy of sildenafil citrate for erectile dysfunction in men with multiple sclerosis: a double-blind, placebo controlled, randomized study. J Urol 2009;181(1):252-8.