What Would You Say? Expressing the Difficulties of Living With Multiple Sclerosis

Selected By
Colleen Harris, MN, NP, MSCN, MSCS
Why is this important to me?
Physical symptoms of MS are visible to others, but some symptoms such as fatigue, pain, depression, and anxiety are less apparent yet equally or more challenging for patients. Because MS is a chronic and unpredictable disease, you may often feel stress. How stress and social support impact coping with the disease is unclear. In general, people are better able to cope with stress from a chronic illness if they have adequate support, because support buffers the negative effects of a disease. Support also allows those with MS to perform activities of daily living despite stress. However, maintaining social interactions can be challenging because of the effort required in managing the disease and its symptom. For some individuals, the difficulty of managing MS and its symptoms can lead to social isolation.
What is the objective of this study?
Patients with MS were asked the open-ended question “If you could communicate to those closest to you (partner, children, friends, etc.) about the emotional difficulties of daily living with MS, what one or two things would you say to them?” Patients were divided into groups according to whether they reported high or low stress and high or low levels of support, and the authors looked for patterns and themes regarding how these factors affected communication about living with the disease.
- Patients with high stress and high support received the highest perceived benefit and total social support. Although their stress was high, the effects of stress were buffered by high support. Their responses to the above question could be summed up as “Please be understanding and patient with me as I am trying to understand my limits and grieve the loss of certain skills. It is unpredictable from day to day”.
- Patients with high stress and low support had the greatest feelings of helplessness and the lowest levels of acceptance of their MS, perceived benefit, total social support, and quality of life. Their response to the above question could be summarized as “If only you could understand what it is like to have MS. I feel uncertain about my disease, my abilities to deal with MS, and the future”.
- Patients with low stress and high support had the highest acceptance of the disease and quality of life and lowest anxiety and depression. Their answer to the above question could be summed up as “It is really frustrating for me to have MS.”
- Finally, patients with low stress and low support reported low quality of life and intermediate levels of anxiety and depression. Their responses to the above question can be summarized as “Be accepting of what I can do. Don’t minimize what I try to do or try to help me too much. Don’t have expectations for me.”
The main themes that emerged from this study were a desire for patients to explain their frustration about physical symptoms to a loved one; the need for support, understanding, and help; and requests for discussion about coping or accepting their disease. This study confirmed the idea that perceived social support buffers the effects of stress by improving the ability to cope. Therefore, if you have high stress but also high support, you are likely to have a higher quality of life and lower anxiety and depression compared to those with high stress but low support. Stress and social support may predict your ability to adjust to MS. Your healthcare provider may be able to suggest stress management interventions and ways to increase your actual and perceived social support.
How did the authors study this issue?
The authors studied the stress levels and the perceived level of support of people with MS and analyzed what patients say to their family members about the emotional problems associated with living with MS. The authors investigated 145 people with MS in Kansas who answered surveys and questions about their stress, support system, coping style, helplessness, acceptance of the disease, quality of life, anxiety, and depression. The authors looked for patterns and themes from these responses. Participants were 73% women, were mostly white, and were an average of 50 years old.
Original Article
What Would You Say? Expressing the Difficulties of Living With Multiple Sclerosis
Journal of Neuroscience Nursing
Jackie Williams Reade, Mark B. White, Carmel Parker White, Candyce S. Russell
ABSTRACT
This article used a mixed method approach to analyze qualitative and quantitative responses from individuals with multiple sclerosis (MS) to determine differences when patients’ perceived stress levels and perceived quality of support are taken into account. Understanding the differences in these responses can help us understand how illness, specifically MS, may influence the relational messages sent by patients to their loved ones. Responses to both quantitative and qualitative questions were obtained from 145 persons who have been diagnosed with MS. Participants responded to scale questions measuring daily stress levels and levels of social support and were divided into four groups on the basis of their scores (low/low, high/low, high/high, and high/low). Thematic analysis was performed on the qualitative responses, and differences were analyzed based on participants’ grouping. Additional outcome variables measuring quality of life, anxiety, depression, helplessness, and acceptance were also analyzed to determine the similarities and differences between the groupings. The information presented in this article both informs and supports the idea that patients’ levels of stress and perception of support are two major variables that impact their responses to their loved ones and their scores on several outcome variables.
Introduction and Literature Review
Chronic illnesses can impact individuals in numerous ways, including increasing the amount of stress they experience and reliance on their social support network. In the following article, individuals’ daily stress level (DSL) and perceived sense of social sup- port are explored to determine how they impact a person’s expression of his or her difficulties of living with multiple sclerosis (MS) to their loved ones. The intent of the article is to determine if DSL and perceived social support are significant variables in determining overall coping for individuals with MS.
MS
MS is an incurable, chronic autoimmune disorder in which myelinVthe protective sheath covering the nerve fibers of the central nervous systemVbecomes damaged and lesions occur (Chelune, Stott, & Pinkston, 2008). These lesions cause disruption of nerve impulses in the brain and spinal cord. Symp- toms of MS can include fatigue, pain, loss of function or feeling in the legs, loss of balance and coordina- tion, slurring of speech, loss of bowel or bladder con- trol, sexual dysfunction, loss of cognitive functioning, and emotional changes (Goodkin, 1992; Mohr & Dick, 1998; Schwartz and Kraft, 1999). Symptoms of MS can appear on a spectrum from mild to crip- pling disability and may take a relapsing-remitting, primary-progressive, or secondary-progressive course (Chelune et al., 2008). In the most common form of MS, relapsing-remitting MS (approximately 85% of newly diagnosed individuals), periods of remission are followed by periods of exacerbations with no way of predicting when remissions will occur or how they will impact the person’s functioning. Primary-progressive MS is characterized by a gradual progression of the disease from its onset without distinct periods of relapse and remission (Chelune et al., 2008). There may be periods of a leveling off of disease activity, and there may be good and bad days or weeks. Secondary-progressive MS begins as a relapsing-remitting form and then changes to a steady progression of clinical neurological damage with or without relapses and minor remissions and plateaus (Chelune et al., 2008). Whereas the physical symptoms of MS are visible and often cause problems with mobility that require the use of assistive devices (e.g., walkers or wheelchairs), other significant symptoms are invisible, such as fatigue, pain, depression, and anxiety. Individuals with MS are reported to have high levels of depressive symptoms (Patten, Metz, & Reimer, 2000) and lower levels of life satisfaction than healthy controls (McCabe, 2002).
Chronic Illness, Uncertainty, and Social Support
Babrow, Hines, and Kasch (2000) argued that the homeostasis and predictability of day-to-day living is disrupted by illness, which results in increased stress. Uncertainty is a significant component of the MS illness experience, as individuals struggle to make sense of the physical, social, emotional, and psy- chological signs that are associated with the illness (Kroencke, Denney, & Lynch, 2001; Radley, 1994). The experience of uncertainty combined with the spec- trum of symptoms associated with MS can affect how individuals interact with their social environment (Wineman, 1990). One element in how uncertainty is managed by individuals with a chronic illness, whether it is reduced, maintained, or increased, de- pends on how the patient perceives social support (Babrow et al., 2000).
Researchers consistently find that people are able to better cope with the stressors that come with a crit- ical or chronic illness when they have a strong sup- port network (Albrecht & Adelman, 1987; Schwarzer & Leppin, 1991). Social support has been found to buffer individuals from negative effects of stress and enhance health and well-being (Goldsmith, 2004). Gulick (2001) found that social support, which in- cluded the presence of emotional and financial sup- port and assistance with tasks, was one factor that allowed people with MS to carry on with activities of daily living (e.g., fine and gross motor skills such as eating, dressing, bathing, walking, traveling; socializing/ recreation; communication; and intimacy) in the midst of the stress associated with the disease. Gulick also indicated that people with MS experience greater reliance on others for support with the worsening of mobility or function as the disease progresses; how- ever, maintaining social connections can be signifi- cantly impaired because of increased effort required in the management of chronic illness (Lyons & Meade, 1995). Social isolation can occur as family and friends may withdraw from the ill person to gain emotional distance, especially when they feel there is nothing they can offer to help. Difficulty with social support can be complicated when individuals with MS feel their illness is being ignored or overemphasized, which can cause them to feel more ill and aware of their illness (Grytten & Maseide, 2006). These stressors can result in negative emotional states that further strain relationships and communication with loved ones.
Perception of Support
Individuals’ perceptions of the availability of others on whom they can rely for support, referred to as ‘‘perceived social support,’’ have proven to be the most consistent and strongest predictor of general personal adjustment for individuals with a chronic illness (Pierce, Sarason, & Sarason, 1996). Simply holding the belief that others will provide appropriate support has been shown to increase patients’ perceived ability to cope with demands, thus lowering stress (Cohen, 1988; Cohen & Wills, 1985; Thoits, 1986; Uchino, Cacioppo, & Kiecolt-Glaser, 1996; Wethington & Kessler, 1986). In the general population, there is substantial evidence that the perceived availability of social support buffers the effect of stress on depression and anxiety (Cohen & Wills, 1985; Dunkel-Schetter & Bennett, 1990; Kawachi & Berkman, 2001; Wills & Shinar, 2000).
Patients receiving social support from their loved ones can be an integral part of a patient’s illness journey (Cohen & Wills, 1985). The structure of individuals’ social networks (Brissette, Cohen, & Seeman, 2000), the support they receive from others (Cohen, Gottlieb, & Underwood, 2000), and the quality and quantity of social interactions (Kiecolt-Glaser & Newton, 2001) have been identified as predictors of health and well-being for both the general population and individuals with an illness. In a study of undergraduates, someone who anticipated that another person would be supportive was more likely to interact with that person to elicit support (Pierce, Sarason, & Sarason, 1992). Wineman (1990) found that people with MS who perceived higher levels of unsupportiveness from loved ones were more likely to feel isolated. The perceptions of availability of so cial support by patients with rheumatoid arthritis were the strongest predictor of their social activity (Curtis, Groarke, Coughlan, & Gsel, 2004).
To date, no published study has analyzed what patients say to their loved ones regarding the emotional difficulties of living with MS. Analyzing their responses and correlating these with their stress levels and perceived levels of support will help further identify factors involved in how patients elicit support and express their emotional difficulties to loved ones. In this study, we sought to better understand the ways stress and perceived support affect what patients with MS say to their loved ones about the emotional difficulties of living with MS. We also wanted to provide qualitative data to complement the existing research and theories regarding perceived support and its stress-buffering effects.
Aim of Study
The purpose of this study was to understand how individuals with MS express their emotional difficulties within the context of family relationship and which factors have the most impact on being able to disclose emotional difficulties to family members. The following research questions were explored using a mixed method design:
(a) Are perceived quality of social support and perceived stress level related to how patients express the emotional aspects of their illness with their loved one(s)?
(b) Can stress and perceived levels of support predict the nature of communication with significant others and family members?
Method
Background
The data analyzed for this study was extracted from a larger mixed method investigation of the experiences of individuals living with MS (cf. Russell, White, & White, 2006), which was approved through the Kansas State University Institutional Review Board. The current study focused on the relationship between perceived social support, DSL, and communication with family members about living with MS.
Procedure
The participants in this study were recruited through the South Central and Western Kansas Chapter of the National Multiple Sclerosis Society (NMSS). The chapter requested a random sample of 1,000 names and addresses affiliated with their chapter from the NMSS database. The initial mailing consisted of a letter introducing the study and a form that potential participants completed, indicating that they had had a definite diagnosis of MS and whether they preferred to complete the study by telephone, the Internet, or a mailed pencil-and-paper survey. Ninety-two of the forms were returned as undeliverable, and 185 individuals returned the form. Of these 185 individuals, two were the family members of MS patients and one had probable MS, and thus, these three were not included in the study. Complete data were obtained from 145 individuals; however, only 103 individuals provided a response to the qualitative questions we focused on in this study. The questions we examined in this study were a small part of a larger study examining a variety of factors related to individuals with MS. See Russell et al. (2006) for a more extensive discussion of the methodology used in the study.
Participants
Seventy-three percent of the participants were women (n = 107). Their ages ranged from 25 to 82 years (median age = 50 years, SD = 11.05 years). In terms of the type of MS, 66% indicated that they had relapsing-remitting MS, 12% had primary-progressive MS, and 9% had secondary-progressive MS. Thirteen percent indicated that they did not know what type of MS they had or selected ‘‘other.’’ Participants had been diagnosed with MS for an average of 10.8 years (range = 1Y38 years). Approximately two thirds of the sample was married (62%), and most did not have children living at home with them (65%). Participants reported household incomes that were fairly evenly scattered across the six income categories (median income range = $40,000Y$59,000) and were an educated group (high school graduate or less, 24%; some college or college graduate, 55%; and some post degree or completed post degree, 21%). Most participants were either on disability (n = 49, 34%) or employed full time (n = 44, 30%). The remaining participants were employed part time (n = 12, 8%), retired (n = 12, 8%), unemployed (n = 8, 6%), full-time homemakers (n = 6, 4%), students (n = 2, 1%), or a combination of one or more of the above. Most identified their religion as either Protestant (60%) or Catholic (14%). Ninety-two percent were European Americans. Thus, the sample was relatively homogeneous with respect to geographic region (Midwestern), religion (Christian), and race (White).
Measures
The larger project from which this study was drawn from assessed a wide range of issues associated living with MS. The assessment battery took individuals approximately 60 minutes to complete. Participants were asked to consider the time frame of the last 4 weeks when contemplating their answers to these questions. The items from the larger project that informed this report included questions about respondents’ perceptions of daily stress, personal coping style, and quality of their support systems. One hundred twenty-seven of the participants completed these questions. First, participants were asked to indicate their self-rated typical DSLs using a 10-point Likert scale with response options ranging from quite minor (1) to mixed (5) to overwhelming (10). Participants were then asked to indicate their perception of the quality of support (QOS) available to them to manage their stress and ability to cope with that stress using a 10-point Likert scale ranging from 1 (not helpful) to 10 (quite helpful). In addition, participants were asked the following open-ended question, ‘‘If you could communicate to those closest to you (partner, children, friends, etc.) about the emotional difficulties of daily living with MS, what one or two things would you say to them?’’
Helplessness, acceptance, and perceived benefit were assessed using the illness cognition questionnaire (Evers et al., 2001). The Multiple Sclerosis Quality of Life-54 Inventory (Vickrey, 1995) was used to measure participants’ quality of life (QOL) and life satisfaction. The Modified MOS Social Support Scale (Rivto et al., 1997) was used to assess perceived social support. The length of diagnosis was calculated as current year minus the year they were diagnosed. Two of the four subscales on the Mental Health Inventory (Veit & Ware, 1983) were used to assess (a) anxiety (‘‘Have you been a very nervous person?’’) and (b) depression (‘‘Have you felt down-hearted and blue?’’).
Qualitative Analysis
Inductive analysis (Miles & Huberman, 1994) was used for analyzing the data. It involves reading and rereading research data to discern emerging categories and the relationships among such categories. Research tactics used included noting patterns and themes in the data, clustering by conceptual grouping, refining emerged concepts and themes with specific details through the process of data reduction, data display, subsuming specific categories into general categories, and conclusion drawing/verification (Miles & Huberman, 1994). Data reduction by coding was performed, and patterns and themes with similar contents were identified. After clustering similar occurrences into patterns, data were displayed in a table to organize the data into clusters and tentative themes, providing a way to make comparisons of similarities and detection of differences and patterns.
After a preliminary examination of the responses, the first author noted patterns and themes in the responses and created conceptual groupings of the messages. To establish interrater reliability for placement of patient-generated responses into the categories, an individual unfamiliar with the research objectives (triangulated researcher) reviewed initial codes and indicated whether or not she agreed with first author. The first author and the triangulated researcher then discussed each of the responses where there was no agreement, until coming to 100% consensus for all responses, sometimes resulting in the renaming of codes. The first author and triangulated researcher made contrasts and comparisons to sharpen conceptual groupings of codes. These codes were subsumed into general categories. The final qualitative analysis tactic utilized was a count of the frequency of various categories within coping groups. Information regarding the categories can be found in Table 3 and will be discussed further in Results. The next stage was conclusion drawing, which involved the primary researcher interpreting and drawing meaning from the data (Miles & Huberman, 1994). During this stage, regularities, patterns, and possible configurations were noted.
Results
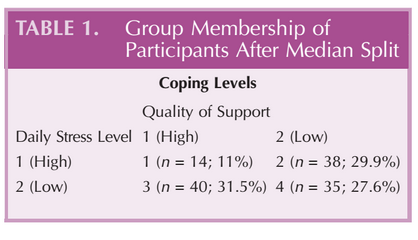
To determine the effects of social support and perceived stress levels on how patients express the emotional difficulties of their illness to loved ones, participants’ responses were transformed into categorical variables to facilitate group comparisons. Median split was used to separate the patients into high and low groups for DSL and QOS on the basis of their responses to Likert scale questions. Coding of variables was performed so that responses associated with low DSL and QOS were scored as 1 and responses associated with high DSL and QOS were scored as 2. Participants’ responses for DSL (n = 127) had a median of 5, a mean of 4.98, and an SD of 1.99. Participants’ responses to QOS (n = 127) had a median of 7, a mean of 6.61, and an SD of 2.25. Participants were divided into four groups along these median scores, which resulted in what we termed as ‘‘coping levels 1Y4.’’ As can be seen in Table 1, individuals who were categorized as 1 had high DSL and high QOS, whereas those categorized as 2 reported high DSL but low QOS.
Analysis of Variance
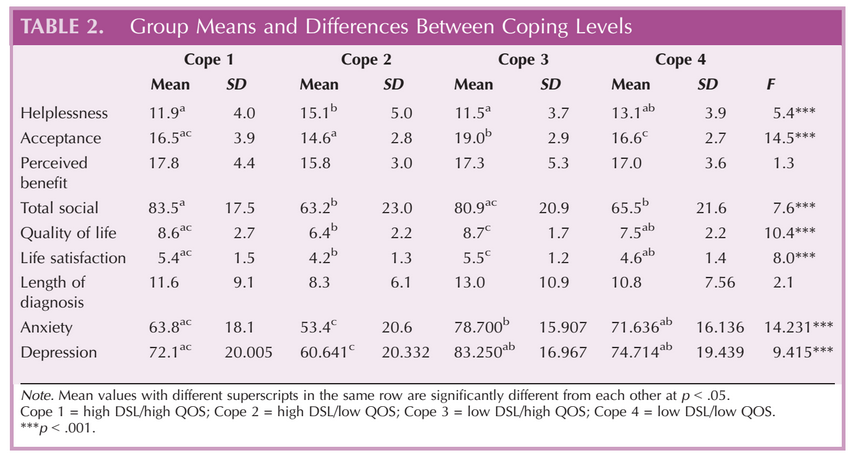
A one-way between-group analysis of variance was conducted to explore the differences in key outcome variables for the four coping groups noted above. Illness-related cognitions (helplessness, acceptance, and perceived benefit), total social support, QOL, life satisfaction, length of diagnosis, and mental health variables (anxiety and depression) were the variables examined to determine the differences between the four coping groups. The two variables of perceived benefit and length of diagnosis were not significant; however, seven of the differences were significant at the p G. 001 level: helplessness, F(3, 134) = 5.44; acceptance, F(3, 131) = 14.51; perceived benefit, F(3, 132) = 1.31; total social support, F(3, 133) = 7.60; QOL, F(3, 126) = 10.43; life satisfaction, F(3, 129) = 7.91; length of diagnosis, F(3, 135) = 2.13; anxiety, F(3, 125) = 14.23; and depression, F(3, 127) = 9.42. Post-hoc comparisons using the Tukey’s test identified those subgroups that were significantly different from each other (see Table 2). In general, the pattern that emerged was the levels of DSL and QOS significantly impacted participants’ scores and could be used to predict scores for various outcome variables, including QOL, helplessness, anxiety, and depression.
Individuals in the cope 1 category (high DSL/high QOS) scored highest of all groups for perceived benefit and total social support. Their scores were second highest in QOL and life satisfaction, whereas their helplessness scores were second lowest of all groups. This group had the third lowest scores of all groups for anxiety and depression. Individuals in this group reported a high DSL; however, the effects of their scores were buffered by their high QOS, as they maintained a high level of QOL and life satisfaction and a low level of helplessness, anxiety, and depression. Those individuals in the cope 2 category (high DSL/low QOS) scored highest of all groups in helplessness and lowest of all groups for acceptance, perceived benefit, total social support, QOL, and life satisfaction, whereas they rated low in acceptance of their MS, overall social support, QOL, and life satisfaction. This group had the highest levels of anxiety and depression among all groups. Individuals in the cope 3 category (low DSL/high QOS) scored highest in acceptance, QOL, and life satisfaction and lowest in anxiety and depression among all the groups. Individuals in the cope 4 category (low DSL/low QOS) did not score the highest or lowest in any outcome variable, although their scores were low for social support, QOL, and life satisfaction. This group had the second lowest levels of anxiety and depression among all groups. Individuals in this group reported low QOS; however, the effects of this score were buffered by their low DSL.
Content Analysis
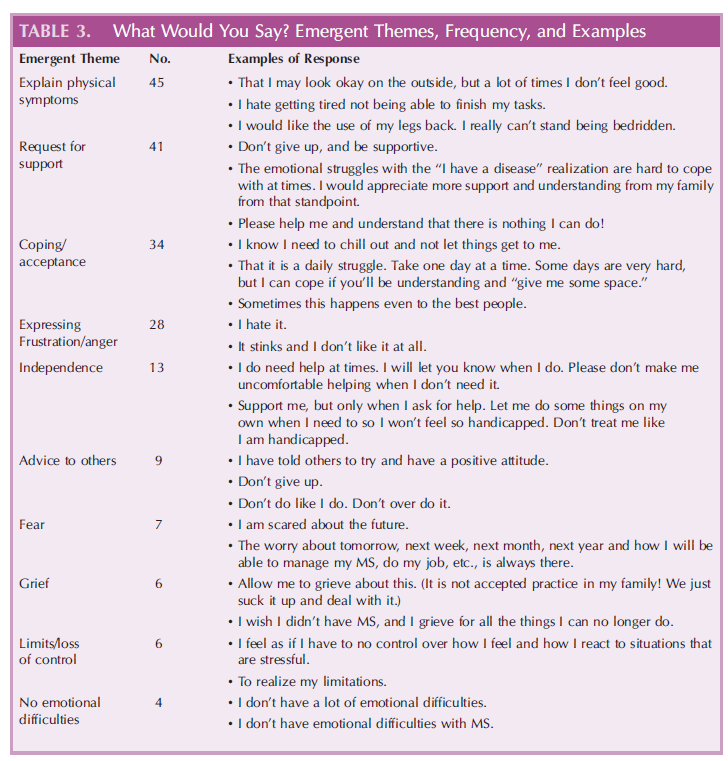
Table 3 illustrates the emergent themes, the frequency that the theme appeared within the responses, and the examples of participants’ responses to the question, ‘‘What would you say to your loved ones about the emotional difficulties of dealing with MS?’’ Eleven themes emerged from the content analysis, wherein one response could be coded as multiple themes.
After clustering coded themes, pattern analysis revealed participants’ responses, primarily wanting to explain their frustration regarding their physical symptoms to a loved one (n = 45). Requests for support, including understanding or help, was the second most common response (n = 41). Discussion of ways the patient coped or worked toward accepting their illness was third most frequent (n = 34). Other prominent responses included expressing frustration or anger about the disease and its limits, requesting the loved one to give him or her more independence, and giving advice to others with MS.
Initially, a meaningful differentiation was hypothesized between responses of those individuals in various coping categories. Although some patterns were noted, the responses did not reveal a significant variation within the coded themes used during this analysis. This discovery was surprising, as this project was undertaken with the assumption that patients with varying levels of support and stress would respond differently when asked to express the emotional difficulties of living with MS to their loved ones. One possible explanation for lack of significant variation could be because of the small number of responses to analyze and misunderstandings on behalf of the participant regarding the meaning of the question. Another possibility is that, despite a patient’s levels of stress and perceived support, the themes of what they wanted to express to a loved one remained constant.
Coping Level Responses
Another method of analysis was undertaken with the data to attempt to inductively discover a way to organize patients’ responses. The primary and triangulated investigator read over responses of patients in coping levels 1, 2, 3, and 4 separately and, after reading each group’s responses, reflected upon a main theme that could sum up the responses within each level. The patients’ responses that were coded as 1 (high DSL/high QOS) were statements that could be summarized as, ‘‘Please be understanding and patient with me as I am trying to understand my limits and grieve the loss
of certain skills. It is unpredictable from day to day.’’ Sample responses from participants in cope 1 included the following:
- ‘‘Be understanding.’’
- ‘‘Allow me to grieve about this.’’
- ‘‘Be patient and realize we can’t do some of the things we used to do.’’
Those responses in group 2 (high DSL/low QOS) often included statements that could be summarized in this way: ‘‘If only you could understand what it is like to have MS. I feel uncertain about my disease, my abilities to deal with MS, and the future.’’ Sample responses from participants in cope 2 included the following:
- ‘‘Walk one day in my shoes and see how difficult it is to live that day.’’
- ‘‘You don’t understand how this affects me.’’
- ‘‘I just wish you could understand or feel what I am feeling.’’
The participants in group 3 (low DSL/high QOS) often responded with statements that could be summarized as, ‘‘It is really frustrating for me to have MS.’’ Sample responses from cope 3 participants included the following:
- ‘‘I would like the use of my legs back. I really can’t stand being bedridden.’’
- ‘‘Took my life I was used to away.’’
- ‘‘My ability to do things does not match my desire. I cannot do everything I would like to do.’’
Finally, respondents in group 4 (low DSL/low QOS) made statements that could be summarized as, ‘‘Be accepting of what I can do. Don’t minimize what I try to do or try to help me too much. Don’t have expectations for me.’’ Sample responses from participants in cope 4 included the following:
- ‘‘Don’t minimize what I accomplish just because you could to the same task and it’s no big deal.’’
- ‘‘Please understand that I need for you not to have the same expectations of me that you do for generally everyone.’’
- ‘‘I do need help at times. I will let you know when I do. Please don’t make me uncomfortable helping when I don’t need it.’’
Discussion
A key theme in the literature on coping is the importance of support provided by other people and how it relates to better illness adjustment (Wineman, 1990). Cohen and Wills (1985) explained the mechanisms by which social relationships influence health outcomes as the stress-buffering model. The stress-buffering model states that perceived social support buffers the effects of stress on individuals by enhancing their coping abilities. Our study confirmed this model as participants who reported high DSL with high QOS rated themselves much better off in areas of QOL, life satisfaction, anxiety, and depression than those with high DSL and low QOS.
In circumstances of illness, Babrow et al. (2000) argued that the equilibrium and predictability of day-to-day living is disrupted, forcing individuals to redefine their identities, and stress increases as a result. How uncertainty is managed, whether it is reduced, maintained, or increased, depends on the assessment of the support recipient, the situation, and the use of appropriate communication skills (Babrow et al., 2000). Our study reflected this as those participants who reported high QOS also reported high QOL and life satisfaction while reporting low scores for anxiety and depression.
The diagnosis of MS consists of challenges in all areas of the biopsychosocial sphere. The experience of MS includes unpredictable and increasing physical symptoms; painful or difficult treatments; and challenges in relationships, career, and daily activities. These elements of illness contribute to increased rates of depression (Janssens et al., 2003), increased anxiety (Zorzon et al., 2001), lower QOL (Janssens et al., 2003), and relationship difficulties (Mohr et al., 1999). In our study, those participants with low DSL reported the lowest levels of depression despite their QOS scores; however, participants with high DSL/high QOS scored similar rates of depression with those with low DSL/low QOS, further indicating the moderating effect social support can have on stress. In regards to anxiety, our study reflected that those who had high DSL/low QOS and high DSL/high QOS reported significantly higher anxiety than their low DSL counterparts.
Illness factors such as length of illness can also affect psychological adjustment in patients with MS (Chwastiak et al., 2002); however, psychological components have been found to more accurately predict differences in individual adjustment (Thomas, Thomas, Hiller, Galvin, & Baker, 2006). A review of the literature regarding psychological correlates of adjustment in patients with MS summarized the findings across studies that high perceived stress was associated with worse adjustment (Dennison, Moss-Morris, & Chalder, 2009). The reporting of perceived life stress has been shown to be strongly associated with depression (Aikens, Fischer, Namey, & Rudick, 1997; Patten et al., 2000). Our study confirmed this in the MS population, as we found that the greatest levels of depression were reported by individuals in the high DSL/low QOS group whereas the lowest levels of depression were reported by those individuals in the low DSL/high QOS group.
Patients’ perceptions of increased psychosocial stressors and decreased social supports have been found to be significantly related to anxiety (Korostil & Feinstein, 2007) and QOL (McCabe & De Judicibus, 2005). A high level of perceived support has also been found as a predictor of adjustment (McCabe, McKern, & McDonald, 2004; Pakenham, 1999). Perceived social support from family members of a patient with MS has also been shown to increase patients’ assessments of their personal, social, and emotional functioning (Krokavcova et al., 2008). A study by Pakenham (1999) indicated that those individuals with MS who perceived their MS-related problems as being highly threatening had differing levels of adjustment, depending on their level of perceived social support. Those with high social support had better social adjustment than those with low social support. For those with low threat appraisals, their social adjustment did not greatly vary.
Our study paralleled these findings in that key outcome variables differed across the four stress level and perceived social support groups. For example, levels of illness-related helplessness showed significant differences among cope 1 and cope 2 categories, which are differentiated by high or low QOS, but maintained the same level of DSLs. QOL and life satisfaction was highest for cope 1 and cope 3, which both reported high QOS. Acceptance of illness was highest for cope 3 and cope 4, which both reported low DSL, whereas cope 1 (high DSL/high QOS) scores for acceptance are almost equal to cope 4 (low DSL/low QOS). Specifically, our findings support the role of perceived stress and social support appraisal in coping and adjustment to MS. Of theoretical significance, our findings suggest that stress and social support variables may predict adjustment to illness and indicate the stress-buffering effects of social support in coping.
Limitations
Our sample was homogenous as it represented Mid-western individuals who were also members of the NMSS of America. Our predominantly White female sample may approach social relationships differently from persons of other racial and ethnic backgrounds. In addition, the number of participants in cope 1 (high QOS/high DSL) was small enough that it may not be a fair representation of that grouping. In addition, our study focused on the responses to one question about communication, and other elements of communication with loved ones were not investigated. Through qualitative analysis, a clear pattern was not well differentiated to hold a substantial value in our findings. Although some patterns began to emerge, there was insufficient qualitative data to see these distinctions more readily.
Implications
Illness shapes communication, from expressing physical pain to expressing the need for support, but little literature exists on how those with illness express themselves to their loved ones and what can be discovered by what they say. This is an area for further study on communication within the social network of those who have MS. Understanding these communication processes can help us understand how illness, specifically MS, influences the individual members and their closest relationships.
In respect to practice implications, the findings suggest the important relationship social support plays in patients coping with MS. The results highlight the need for medical professionals to inquire about social support and perceived stress levels as indicators of coping with the physical and psychosocial implications of MS. Providing stress management interventions that reduce perceived stress, as well as assisting patients in finding ways to maximize their perceived and actual social support, is recommended. Although findings do not directly address the impact of support from clinicians on the medical team, it may have similar positive effects on patient coping. Future research should be conducted regarding the impact social support from the patient’s social context and the medical team has on individuals coping with MS. Exploring and determining best practices for teaching skills in providing support for patients with MS can increase the likelihood that patients experience an increase in coping abilities.
References
Aikens, J., Fischer, J., Namey, M., & Rudick, R. (1997). A replicated prospective investigation of life stress, coping, and depressive symptoms in multiple sclerosis. Journal of Behavioral Medicine, 20, 433Y445.
Albrecht, T., & Adelman, M. (1987). Communicating social support: A theoretical perspective. In T. L. Albrecht & M. B. Adelman (Eds.), Communicating social support (pp. 18Y39). Newbury Park, CA: Sage.
Babrow, A., Hines, S., & Kasch, C. (2000). Illness and uncertainty: Problematic integration and strategies for communicating about medical uncertainty and ambiguity. In B. B. Whaley (Ed.), Explaining illness: Messages, strategies and concepts (pp. 41Y67). Hillsdale, NJ: Lawrence Erlbaum.
Brissette, I., Cohen, S., & Seeman, T. E. (2000). Measuring social integration and social networks. In S. Cohen, L. Underwood, & B. Gottlieb (Eds.), Social support mea-
surement and intervention (pp. 53Y85). New York, NY: Oxford University Press.
Chelune, G., Stott, H., & Pinkston, J. (2008). Multiple sclerosis. In J. E. Morgan & J. H. Ricker (Eds.), Textbook of clinical neuropsychology (pp. 599Y615). New York, NY: Taylor & Francis.
Chwastiak, L., Ehde, D., Gibbons, L., Sullivan, M., Bowen, J., & Kraft, G. (2002). Depressive symptoms and severity of illness in multiple sclerosis: Epidemiologic study of a large community sample. American Journal of Psychiatry, 159, 1862Y1868.
Cohen, S., & Wills, T. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310Y357.
Cohen, S. (1988). Psychosocial models of social support in the etiology of physical disease. Health Psychology, 7, 269Y297.
Cohen, S., Gottlieb, B., & Underwood, L. (2000). Social relationships and health. In S. Cohen, L. Underwood, & B. Gottlieb (Eds.), Measuring and intervening in social support (pp. 3Y25). New York, NY: Oxford University Press.
Curtis, R., Groarke, A., Coughlan, R., & Gsel, A. (2004). The influence of disease severity, perceived stress, social support and coping in patients with chronic illness: A 1 year follow up. Psychology, Health and Medicine, 9, 456Y475.
Dennison, L., Moss-Morris, R., & Chalder, T. (2009). A review of psychological correlates of adjustment in patients with multiple sclerosis. Clinical Psychology Review, 29, 141Y153.
Dunkel-Schetter, C., & Bennett, T. L. (1990). Differentiating the cognitive and behavioral aspects of social support. In B. R. Sarason, I. G. Sarason, & G. R. Pierce (Eds.), Social support: An interactional view, (pp. 267Y296). New York, NY: John Wiley & Sons.
Evers, A., Kraaimaat, F., van Lankveld, W., Jongen, P., Jacobs, J., & Bijlsma, J. (2001). Beyond unfavorable thinking: The Illness Cognition Questionnaire for chronic diseases. Journal of Consulting and Clinical Psychology, 69(6), 1026Y1036.
Goldsmith, D. J. (2004). Communicating social support. Cambridge, England: Cambridge University Press.
Goodkin, D. E. (1992). The natural history of multiple sclerosis. In R. A. Rudick & D. E. Goodkin (Eds.), Treatment of multiple sclerosis: Trial design, results and future perspectives (pp. 17Y46). New York, NY: Springer-Verlag.
Grytten, N., & M*seide, P. (2006). ‘‘When I am together with them I feel more ill’’: The stigma of multiple sclerosis experienced in social relationships. Chronic Illness, 2, 195Y208.
Gulick, E. E. (2001). Emotional distress and activities of daily living functioning in persons with multiple sclerosis. Nursing Research, 50, 147Y154.
Miles, M. B., & Huberman, A. M. (1994). Data management and analysis methods. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of qualitative research, (pp. 428Y444). Thousand Oaks, CA: Sage Publications.
Janssens, A., van Dorn, P., de Boer, J., van der Meche, F., Passchier, J., & Hintzen, R. (2003). Impact of recently diagnosed multiple sclerosis on quality of life, anxiety, depression and distress of patients and partners. Acta Neurologica Scandinavica, 108, 389Y395.
Kawachi, I., & Berkman, L. (2001). Social ties and mental health. Journal of Urban Health: Bulletin of the New York Academy of Medicine, 78, 458Y467.
Kiecolt-Glaser, J. K., & Newton, T. L., (2001). Marriage and health: His and hers. Psychological Bulletin, 127, 472Y503.
Korostil, M., & Feinstein, A. (2007). Anxiety disorders and their clinical correlates in multiple sclerosis patients. Multiple Sclerosis, 13, 67Y72.
Kroencke, D. C., Denney, D. B., & Lynch, S. G. (2001). Depression during exacerbations in multiple sclerosis: The importance of uncertainty. Multiple Sclerosis, 7, 237Y242.
Krokavcova, M., van Dijk, J. P., Nagyova, I., Rosenberger, J., Gavelova, M., Middel, B., Gdovinova, Z., & Groothoff, J. (2008). Social support as a predictor of perceived health status in patients with multiple sclerosis. Patient Education and Counseling, 73, 159Y165.
Lyons, R., & Meade, D. (1995). Painting a new face on relationships: Relationship remodeling in response to chronic illness. In S. Duck & J. Wood (Eds.), Confronting relationship challenges (pp. 181Y210). Thousand Oaks, CA: Sage Publications.
McCabe, M. P. (2002). Relationship functioning and sexuality among people with multiple sclerosis. The Journal of Sex Research, 39, 302Y309.
McCabe, M., & De Judicibus, M. (2005). The effects of economic disadvantage on psychological well-being and quality of life among people with multiple sclerosis. Journal of Health Psychology, 10, 163Y173.
McCabe, M., McKern, S., & McDonald, E. (2004). Coping and psychological adjustment among people with multiple sclerosis. Journal of Psychosomatic Research, 56, 355Y361.
Mohr, D., & Dick, L. (1998). Multiple sclerosis. In P. M. Camic & S. Knight (Eds.), Clinical handbook of health psychology: A practical guide to effective interventions (pp. 313Y348). Seattle, WA: Hogrefe & Huber.
Mohr, D., Dick, L., Russo, D., Pinn, J., Boudewyn, A., & Goodkin, D. (1999). The psychosocial impact of multiple sclerosis: Exploring the patient’s perspective. Health Psychology, 18, 376Y382.
Pakenham, K. (1999). Adjustment to multiple sclerosis: Application of a stress and coping model. Health Psychology, 18, 383Y392.
Patten, S., Metz, L., & Reimer, M. (2000). Biopsychosocial correlates of lifetime major depression in a multiple sclerosis population. Multiple Sclerosis, 6, 115Y120.
Pierce, G., Sarason, B., & Sarason, I. (1992) General and specific support expectations and stress as predictors of perceived supportiveness: An experimental study. Journal of Personality and Social Psychology, 63, 297Y307.
Pierce, G., Sarason, B., & Sarason, I. (1996). Handbook of social support and the family. New York, NY: Plenum Press.
Radley, A. (1994). Making sense of illness: The social psychology of health and disease. Thousand Oaks, CA: Sage Publications.
Rivto, P. G., Fischer, J. S., Miller, D. M., Andrews, H., Paty, D.
W., & LaRocca, N. G. (1997). The Multiple Sclerosis Quality of Life Inventory: A user’s manual. New York, NY: National Multiple Sclerosis Society.
Russell, C., White, M., & White, C. (2006). Why me? Why now? Why multiple sclerosis?: Making meaning and perceived quality of life in a Midwestern sample of patients with mul-
tiple sclerosis. Families, Systems, & Health, 24(1), 65Y81.
Schwartz, L., & Kraft, G. H. (1999). The role of spouse responses to disability and family environment in multiple sclerosis. American Journal of Medical Rehabilitation, 78, 525Y532.
Schwarzer, R., & Leppin, A. (1991). Social support and health: A theoretical and empirical overview. Journal of Social and Personal Relationships, 8, 99Y127.
Thoits, P. (1986). Social support as coping assistance. Journal of Consulting and Clinical Psychology, 54, 416Y423.
Thomas, P., Thomas, S., Hiller, C., Galvin, K., & Baker, R. (2006). Psychological interventions for multiple sclerosis (Review). Cochrane Database of Systematic Reviews, 1, CD004431. doi:10.1002/14651858.CD004431.pub2
Uchino, B., Cacioppo, J., & Kiecolt-Glaser, J. (1996). The relationship between social support and physiological processes: A review with emphasis on underlying mechanisms and Implications for health. Psychological Bulletin, 119, 488Y531.
Vickrey, B. G. (1995). Multiple Sclerosis Quality of Life (MSQOL)-54 Instrument. Los Angeles, CA: University of California at Los Angeles.
Veit, C., & Ware, J. (1983). The structure of psychological distress and well-being in general populations. Journal of Consulting and Clinical Psychology, 51, 730Y742.
Wethington, E., & Kessler, R. (1986). Perceived support, received support, and adjustment to stressful life events. Journal of Health and Social Behavior, 27, 78Y89.
Wills, T. A., & Shinar, O. (2000). Measuring perceived and received social support. In S. Cohen, L. G. Underwood, & B. H. Gottlieb (Eds.), Social support measurement and intervention: A guide for health and social scientists (pp. 86Y135). New York, NY: Oxford University Press.
Wineman, N. (1990). Adaptation to multiple sclerosis: The role of social support, functional disability and perceived uncertainty. Nursing Research, 39, 294Y299.
Zorzon, M., de Masi, R., Nasuelli, D., Ukmar, M., Pozzi Mucelli, R., Cazzato, G., I Zivadinov, R. (2001). Depression and anxiety in multiple sclerosis: A clinical and MRI study in 95 subjects. Journal of Neurology, 248, 1432Y1459.