Relationship Among MS, Sleep Quality, and Sleep Hygiene Behaviors
Why is this important to me?
Poor-quality sleep not only affects our ability to focus at work and care for our families, it can also lead to cognitive decline. Current studies indicate that fatigue and poor sleep occur in more than 80% of people with MS. It is believed that MS-related fatigue can be caused by the disease as well as other related conditions, such as anxiety, depression, disordered sleep, or various side-effects from medication
This study examines the relationship among anxiety, difficulty concentrating, sleep hygiene, and sleep quality in adults with MS who self-report fatigue.
How did the authors study this issue?
The authors recruited 39 adults diagnosed with relapsing-remitting MS or secondary progressive MS between the ages of 18 and 70. Participants were asked to participate in a survey by answering questions pertaining to sleep quality and sleep behaviors. In addition to the survey, participants were asked to log a diary each morning on the previous night’s sleep quality and their associated sleep behaviors.
To assess sleep quality, the authors used the Pittsburgh Sleep Quality Index (PSQI), which includes 7 elements of sleep quality such as:
- Subjective sleep quality
- Sleep latency
- Sleep duration
- Habitual sleep efficiency
- Sleep disturbances
- The use of sleep-promoting medications
- Daytime dysfunction
To assess sleep behavior, participants were asked to rate (from never to very often) how often they engaged in certain behaviors around bedtime during an average week. Behaviors included:
- Watching TV
- Listening to the radio
- Reading
- Smoking
- Talking to someone
- Eating or drinking
What did this study show?
This study indicated that poor sleep behaviors (“poor sleep hygiene”), including watching TV, talking on the phone, and listening to the radio was significantly connected to reports of fatigue. The study concluded that the use of technology impacted sleep quality and it was recommended participants remove electronic devices such as TV and phones from the bedroom and restrict usage at least one hour before bedtime. The authors also concluded that symptoms of forgetfulness, anxiety, and difficulty concentrating were significantly correlated to sleep quality.
The important message in this study for people with MS is that sleep quality matters a great deal to their overall sense of well-being as well as their success in modifying the impact of this disease. If a good night’s sleep is important for everyone, good sleep quality is essential for people with MS. If you believe that you are not sleeping as well as you should, mention it to your healthcare provider. They can help you to understand what may be preventing you from sleeping and recommend ways to improve your sleep quality.
Original Article
The Relationship Among Multiple Sclerosis–Related Symptoms, Sleep Quality, and Sleep Hygiene Behaviors
Pamela Newland, Rebecca A. Lorenz, Judith M. Smith, Emily Dean, John Newland,
Patricia Cavazos
Journal of Neuroscience Nursing
Abstract
The aim of this study was to examine the relationships among multiplesclerosis (MS)–related symptoms, sleep hygiene behaviors, and sleep quality in adults with MS who self-report fatigue.
Background: Fatigue is a frequent, prevalent symptom among adults with MS. Few studies have examined the relationship among fatigue and other symptoms with sleep quality and sleep behaviors.
Design: This is a descriptive correlational study.
Methods: A convenience sample of 39 adults with MS were recruited for the study. Instruments used included the revised MS Related Symptom Scale and the Pittsburgh Sleep Quality Index. Correlations examined the relationships among fatigue and other MS symptoms with sleep quality and sleep hygiene behaviors.
Results: The frequency of several symptoms correlated with poor sleep quality, and fatigue frequency was higher in those who used electronic devices and practiced poor sleep hygiene behaviors.
Nursing Implications: Nurses should incorporate interventions for symptoms that impact sleep quality. These findings suggest that sleep hygiene education should be a part of routine clinical care.
Conclusion: Adults with MS experience the burden of many symptoms that impact sleep quality. Interventions that include education to improve symptoms, sleep hygiene behaviors, and sleep quality are needed.
Multiple sclerosis (MS) is a central nervous system (CNS) disease leading to inflammation and demyelination of the brain and spinal cord. This debilitating neurological disorder affects an estimated 2.3 million adults worldwide and is the leading cause of loss of work and disability among young adults.1,2 In addition to the neurological disease, MS is associated with several symptoms including disordered sleep that impacts overall well-being and quality of life (QOL). Signs and symptoms of MS depend on the location of the CNS affected; however, fatigue is themost common symptom of MS.3
Fatigue in MS4 can be caused either by the disease itself or as a result of other symptoms such as anxiety, depression, disordered sleep, or various medication regimens. Approximately 60% to 90% of people with MS complain of fatigue, and there is evidence that disordered sleep and depression are contributing factors.5,6 It has been suggested that MS-related fatigue is both primary and secondary, with disordered sleep worsening fatigue by overstimulating the CNS. The etiology remains uncertain, but extreme triggering of the CNS may cause disruption in circadian rhythm leading to increase in fatigue severity. Fatigue leads to decreased QOL by impeding activities of daily living and reducing psychological well-being and ability to work.4
Fatigue in adults with MS can be affected by not only poor sleep quality but also anxiety and depression, which are also common.7–9 In fact, anxiety can occur in approximately 30% of people with MS.9 The stressors of the MS diagnosis can impact people because of the cumbersome disease sequelae, such as unpredictable relapses, complicated medication regimes, and multiple psychosocial issues.10 People with MS struggle daily with a multitude of symptoms, including pain, fatigue, cognitive issues, depression, and anxiety.9,11
Poor sleep hygiene is a set of behaviors that influence sleep quality (ie, watching television [TV], uncomfortable nighttime ambient temperature, and exciting presleep activities). These behaviors have been found to be more prevalent among poor sleepers.12 There is some evidence of a relationship between fatigue and sleep qualityamong adults with MS. A few studies have suggested that sleep quality is connected to increased disability13 and cognitive decline (sustained working memory)14 and global cognitive performance, which can decrease QOL and theability to conduct work-related tasks.
Fatigue and disordered sleep are a public health problem, and existing studies and education are lacking for those with MS. To our knowledge, no one has explored the relationship among fatigue, MS symptoms, and sleep hygiene behaviors. Therefore, the purpose of this study was to examine the relationship among anxiety, difficulty concentrating, sleep hygiene behaviors, and sleep quality in adults with MS who self-report fatigue.
Method
The survey questions were developed to be completed by the participants in their desired setting (home, library) via computer, tablet, or other mobile devices with phone assistance available, if needed, from the primary investigator or research assistant. A computer programmer collaborated with the research team to develop the questionnaire within REDCap, a secured web environment. Next, interviews were conducted with 5 participants to ask for input on diary questions for the final version to be sent to a target of 30 participants with MS. Each subject received a web link through text message for detailed instructions and questions via REDCap.15
Sample
We recruited a convenience sample of community-dwelling adults from MS clinics in the midwestern United States during routine clinic appointments and from a local MS society’s listserv. The inclusion criteria were a definitive diagnosis of relapsing-remitting MS or secondary progressive MS, age of 18 to 70 years, willingness to write about symptoms and lifestyle habits in a web-based diary format, reliable computer and Internet access, and ability to read and speak English.
Procedures
We obtained the university’s institutional review board approval. Written consent was obtained from all participants during a private face-to-face clinic visit once all questions were answered, and participants were assured of confidentiality and ability to withdraw at any time without consequence. After consent, participants who volunteered for the study completed a demographic form and were instructed how to use REDCap and provided instructions on completion of the web-based diary. Participants were asked to log into REDCap once a day for 7 consecutive days to answer narrative questions in the electronic diary regarding symptoms that positively or negatively impacted sleep and lifestyle habits. After 4 weeks, the subject was asked to repeat the survey for 7 more days. Data were collected for 7 consecutive days; however, because the primary aim was to examine feasibility of the data collection method, 4 days of electronic diary data were accepted as full participation in this study.
Measures
Demographics
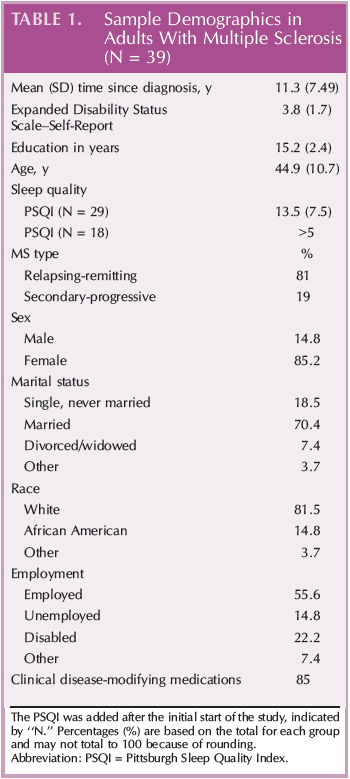
Self-reported demographic information was obtained included age, race, sex, education, marital status, and disease-modifying therapy use (yes/no). Disease-modifying therapy use was validated through review of medical records.
MS Related Symptom Scale (Revised)
We obtained symptoms experienced using a revised version of the MS Related Symptom Scale,16 with additional items generated from focus group data,5 and a single open-ended question to gather recent co-occurring symptoms(total, 37 items). Symptom frequency was reported on a 6-point scale from 0 (never) to 5 (always), with a total score ranging from 0 to 180 (higher score = higher frequency). The test-retest reliability was excellent at 0.89.2,5
Expanded Disability Status Scale: Patient Version
The patient self-report version of the Expanded Disability Status Scale (EDSS) provided an estimate of disability status.17 The scale is composed of 17 items that mirror the physician-administered EDSS and has been found to be highly reliable with Cronbach’s alpha of 0.92. Summing the scores provides a possible range of 0 (normal neurological examination) to 10 (death due to MS).
Sleep Quality (Single-Item Scale)
All participants rated the previous night’s sleep quality every morning on a visual analog scale from 1 to 10 (extremely poor to extremely good). Test-retest reliability coefficients of the Sleep Quality visual analog scale have been found to range from 0.91 to 0.90.18
Pittsburgh Sleep Quality Index
We used the Pittsburgh Sleep Quality Index (PSQI)19 to assess self-reported sleep quality. The PSQI includes 19 items creating 7 dimensions of sleep quality (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, the use of sleep-promoting medication, and daytime dysfunction). Each dimension was scored using a scale of 0 (not during the past month) to 3 (3 or more times per week) with a global sum of 5 or greater indicating poor sleep quality. Cronbach’s α is .83 for its 7 components.19 The instrument takes approximately 5 to 10 minutes to complete.
Sleep Behavior Self-Rating Scale
Participants rated during an average week how often they did certain behaviors around bedtime from never to very often.20 Behaviors included watching TV, listening to the radio, reading, smoking, talking to someone, and eating or drinking. The instrument has a high test-retest reliability (r = 0.88) and internal consistency (Cronbach’s α of .76).
Data Analysis
Descriptive statistics for continuous variables (mean, median, range, and standard deviation) were obtained for thesample. Frequency was tabulated for categorical variables. Symptom variables were computed using ordinal scale. The outcome variables were PSQI total scores, and the demographic variables were age and sex. Modeling was performed using PROC GLIMMIX in SAS. All analyses were 2-sided with a significance level of .05. Statistical analyses were performed using SAS 9.4.
Results
Characteristics of the Participants
The sample was composed of 39 participants with MS. Demographic and related clinical data are shown in Table 1. Most participants were female (85%) and white (81%). The subtype of MS was mainly relapsing-remitting MS (81%) with a mean (SD) time since diagnosis of 11.3 (7.5) years, and the mean (SD) EDSS (self-report version) was 3.8 (1.7), suggesting a lower level of disability (Table 1). Correlations did not reveal differences in age, education, length since diagnosis, MS relapse, disability status, or sleep variables from the PSQI.
Correlation Analysis
The frequencies of forgetfulness, anxiety, and difficulty concentrating were significantly correlated with sleep quality. Separate components of the PSQI were examined as predictors of sleep, in which 3 symptoms (forgetfulness, anxiety, and difficulty concentrating) were statistically significant predictors (P < .5). The remaining components were not associated with sleep (fatigue [P = .05], pain [P = .10], and heat intolerance [P = .25]).
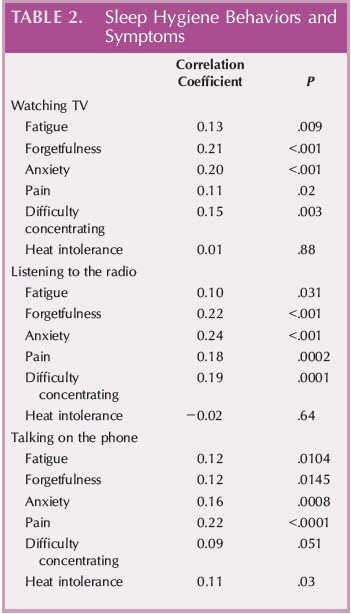
In contrast, fatigue, pain, and heat intolerance frequencies were not associated with sleep quality on the PSQI. Sleep behaviors including watching TV, talking on the phone, and listening to the radio significantly correlated with frequent reports of fatigue, forgetfulness, anxiety, and pain. In addition, watching TV and listening to the radio, but not talking on the phone, were significant for frequent reports of difficulty concentrating. Notably, talking on thephone was significantly associated with heat intolerance (Table 2). For the symptoms and demographic variables, there were significant differences for fatigue frequency and sex (P < .007).
Discussion
This article investigated self-report fatigue frequency and other symptoms with sleep quality and sleep hygiene behaviors in adults with MS. Our findings indicated that MS symptoms, including fatigue, are related to poor sleep hygiene behaviors, which corresponds with existing studies that indicate fatigue and poor sleep occur in more than 80% of the patients with MS.3,21 This is a concern because fatigue and poor sleep often cluster with a cycle of depression, anxiety, and difficulty concentrating.5,22 We found that psychological problems, including forgetfulness, anxiety, and difficulty concentrating, are also correlated with sleep quality. Our findings are significant for corroborating existing studies on the high prevalence of sleep problems among patients with MS. Furthermore, our findings signal the cascading of psychological problems and a need for mental health screening and intervention, especially when patients with MS present with sleep difficulties.
Forgetfulness, anxiety, and difficulty concentrating were symptoms that correlated with sleep quality. Previous studies found that anxiety and poor sleep demonstrated a strong relationship to overall worry about health.23,24Reduced sleep quality is a severe problem for patients with MS and could negatively impact the patients’ overall health. Furthermore, cognitive impairment and altered moods can manifest in those with difficulty sleeping. 13Depression and anxiety are both considered mood disorders, often overlapping. Excessive worry, indicative of an anxiety spectrum disorder, is not only related to impaired health, but this relationship is bidirectional.23 Moreover, fatigue, anxiety, poor sleep quality, and, ultimately, sleep hygiene behaviors may factor into this problem. It is unclear why these symptoms cluster together.
Inconsistent with others,2,21 pain was not significantly related with poor sleep quality. It may be that pain was underreported because of the severity of fatigue and other symptoms. It was not possible, however, to glean from this study because of lack of causation and the use of the revised version of the MS Related Symptom Scale, because it has only 1 item for pain frequency. Our findings suggest a need for further exploration and development of how symptoms are related, which would ultimately impact the lives of adults living with MS. Because fatiguefrequency and sleep quality are subjective symptoms, the 2 symptoms are better assessed as separate concepts.
This study found that use of technology was related to sleep quality. These findings support the National Sleep Foundation’s25 recommendation to remove electronic devices, such as TV and phones, from the bedroom and restrict use during the hour before bedtime.26 The use of technology before bedtime has been found to be associated with increased mood disturbances.27 However, there has been little research on adults and, to our knowledge, none on adults with MS. There is some evidence suggesting that the combined use of mobile and computer use is associated with perceived stress, symptoms of anxiety and depression, and sleep disturbances among college-aged adults.28 Future studies should examine the underlying relationships between evening electronic device use, stress, sleep, and depression among adults.
Limitations
It is important to acknowledge the small sample size. In addition, because of the descriptive study design, it is not possible to establish causality, for example, between symptom pathology (eg, difficulty concentrating) and sleep quality. Thus, study results might not represent populations with greater odds of poor sleep quality due to increased disability. These results should be interrupted judiciously because of self-report of symptom frequency and sleep quality. Although both the MS-RS and the PSQI are well-validated tools for measuring symptoms and sleep quality, individual symptoms of anxiety and depression were not initially assessed for clinical depression or anxiety. Future studies may benefit from inclusion of well-validated tools recommended by the American Academy of Neurology (eg, Patient Health Questionnaire-9/Neuro QOL for depression and the Generalized Anxiety Disorder-7 for anxiety)29 to establish a baseline and tease out subjective perceptions of the adults with MS.
Nursing Implications and Future Directions
Our findings suggest that interventions aimed to improve sleep hygiene may also reduce anxiety, fatigue, and forgetfulness, which are common MS symptoms. Other interventions, such as cognitive behavioral therapy for insomnia, ought to be considered. At a minimum, these findings stress a need for comprehensive screening and assessment of multiple symptoms at each encounter such as a criterion standard fatigue assessment, with those of anxiety, sleep quality, or forgetfulness.29,30 Nurses caring for patients with MS should educate them about successful coping skills and strategies with fatigue and sleep, especially for those who are prone to anxiety and worry. Future studies would be strengthened by using a combination of self-report and objective measures of sleep (eg, polysomnography, wrist actigraphy) in a larger sample of patients with MS.
Conclusion
This study examined the relationship among fatigue, symptoms, sleep hygiene, and sleep quality in adults with MS. The findings suggest that several symptoms are still in need of assessment and screening to support improved sleep quality among adults with MS. In addition, education is needed on sleep hygiene measures to improve overall sleep. Future investigations of symptoms and sleep are needed, especially randomized efforts aimed at improving anxiety and depression and supporting sleep quality.
Acknowledgments
The authors thank Angela Spencer, MLS, AHIP Health Sciences Librarian, Goldfarb School of Nursing.
References
1. Kister I, Bacon TE, Chamot E, et al. Natural history of multiple sclerosis symptoms. Int J MS Care. 2013;15(3):146Y158.
2. Newland P, Riley M, Foerster LA, Thomas FP. Relation of demographics and reported symptoms and medication use in persons with multiple sclerosis. Medsurg Nurs. 2015;24(5):336Y341.
3. Boe Lunde HM, Aae TF, Indrev*g W, et al. Poor sleep in participantswithmultiple sclerosis. PLoS One. 2012;7(11):e49996.
4. Berger JR, Pocoski J, Preblick R, Boklage S. Fatigue heralding multiple sclerosis. Mult Scler. 2013;19(11):1526Y1532.
5. Newland P, Fearing A, Riley M, Neath A. Symptom clusters in womenwith relapsing-remitting multiple sclerosis.J Neurosci Nurs. 2012;44(2):66Y71.
6. Nociti V, Losavio FA, Gnoni V, et al. Sleep and fatigue in multiple sclerosis: a questionnaire-based, cross-sectional, cohort study. J Neurol Sci. 2017;372:387Y392.
7. Amato MP, Ponziani G, Rossi F, Liedl CL, Stefanile C, Rossi L. Quality of life in multiple sclerosis: the impact of depression, fatigue and disability. Mult Scler J. 2001; 7(5):340Y344.
8. Berzins SA, Bulloch AG, Burton JM, Dobson KS, Fick GH, Patten SB. Determinants and incidence of depression in multiple sclerosis: a prospective cohort study. J Psychosom Res. 2017;99:169Y176.
9. Gay MC, Bungener C, Thomas S, et al. Anxiety, emotional processing and depression in people with multiple sclerosis. BMC Neurol. 2017;17(1):43.
10. Hartoonian N, Terrill AL, Beier ML, Turner AP, Day MA, Alschuler KN. Predictors of anxiety in multiple sclerosis. Rehabil Psychol. 2015;60(1):91Y98.
11. Hughes AJ, Turner AP, Alschuler KN, et al. Association between sleep problems and perceived cognitive dysfunction over 12 months in individuals with multiple sclerosis. Behav Sleep Med. 2018;16(1):79Y91.
12. Gellis LA, Lichstein KL. Sleep hygiene practices of good and poor sleepers in the United States: an Internet-based study. Behav Ther. 2009;40(1):1Y9.
13. VitkovaM, Gdovinova Z, Rosenberger J, et al. Is poor sleep quality associated with greater disability in patients with multiple sclerosis? Behav Sleep Med. 2018;16(2):106Y116.
14. Van Geest Q, Westerik B, van der Werf YD, Geurts JJ, Hulst HE. The role of sleep on cognition and functional connectivity in patients withmultiple sclerosis.J Neurol. 2017;264(1):72Y80.
15. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)Vametadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377Y381.
16. Gulick EE. Model confirmation of the MS-Related Symptom Checklist. Nurs Res. 1989;38(3):147Y153.
17. Bowen J, Gibbons L, Gianas A, Kraft GH. Self-administered Expanded Disability Status Scale with functional system scores correlates well with a physician-administered test. Mult Scler. 2001;7(3):201Y206.
18. Cappelleri JC, Bushmakin AG, McDermott AM, Sadosky AB, Petrie CD, Martin S. Psychometric properties of a single-item scale to assess sleep quality among individualswith fibromyalgia. Health Qual Life Outcomes. 2009;7:54.
19. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193Y213.
20. Kazarian SS, Howe MG, Csapo KG. Development of the Sleep Behavior Self-Rating Scale. Behav Ther. 1979;10(3):412Y417.
21. Amtmann D, Askew RL, Kim J, et al. Pain affects depression through anxiety, fatigue and sleep in multiple sclerosis. Rehabil Psychol. 2015;60(1):81Y90.
22. Motl RW, Suh Y, Weikert M. Symptom cluster and quality of life in multiple sclerosis. J Pain Symptom Manage. 2010;39(6):1025Y1032.
23. Jones SM, Amtmann D. Health care worry is associatedwith worse outcomes in multiples sclerosis. Rehabil Psychol.2014;59(3):354Y359.
24. Braley TJ, Kratz AL, Kaplish N, Chervin RD. Sleep and cognitive function in multiple sclerosis. Sleep. 2016;39(8):1525Y1533.
25. National Sleep Foundation. Multiple sclerosis and sleep. Available at http://sleepfoundation.org/sleep-disordersproblems/multiple-sclerosis-and-sleep. Accessed July 3, 2018.
26. Fossum IN, Nordnes LT, Storemark SS, Bjorvatn B, Pallesen S.The association between use of electronic media in bed before going to sleep and insomnia symptoms, daytime sleepiness, morningness, and chronotype. Behav Sleep Med. 2014;12(5):343Y357.
27. Adams SK, Kisler TS. Sleep quality as a mediator between technology-related sleep quality, depression, and anxiety. Cyberpsychol Behav Soc Netw. 2013;16(1):25Y30.
28. Thom2e S, EklPf M, Gustafsson E, Nilsson R, Hagberg M. Prevalence of perceived stress, symptoms of depression and sleep disturbances in relation to information and communication technology (ICT) use among young adults Van explorative prospective study. Comput Human Behav. 2007;23(3): 1300Y1321.
29. Minden SL, Feinstein A, Kalb RC, et al. Guideline Development Subcommittee of the American Academy of Neurology. Evidence-based guideline: assessment and management of psychiatric disorders in individuals with MS: Report of the Guideline Development Subcommittee of the American
Academy of Neurology. Neurology. 2014;82(2):1Y8.
30. Edwards KA, Molton IR, Smith AE, et al. Relative importance of baseline pain, fatigue, sleep, and physical activity: predicting change in depression in adults with multiple sclerosis. Arch Phys Med Rehabil. 2016;97(8):1309Y1315