Psychobehavioral Treatment Options for Sexual Dysfunction in Multiple Sclerosis: A Systematic Review
Why is this study important?
Multiple sclerosis (MS) causes various impairments that may affect quality of life. Among these, sexual dysfunction occurs in up to 75% of people with MS, and is often present in the early stages of the disease. People with MS may experience a wide range of issues, including decrease in libido and vaginal lubrication, erectile dysfunction, and difficulties with orgasm.
Although sexual dysfunction is a significant impairment that has been shown to worsen the psychological impact of MS, it is only rarely mentioned during health care visits. Because time is limited during these visits, discussions between people with MS and their health care providers tend to focus on neurologic deficits that are perceived as severe and potentially disabling. Moreover, both health care providers and individuals with MS are often reluctant to tackle the topic of intimacy in the presence of partners, family members, or caregivers.
Studies have shown that medications are not a one-size-fits-all solution for treating problems related to sexual function or improving sexual satisfaction in people with MS, partly because these individuals may experience many different types and degrees of sexual dysfunction. The therapies that have been used in individuals with MS are generally targeted toward the type of sexual dysfunction resulting directly from MS-related lesions in the brain or spinal cord areas involved in sexual response (primary sexual dysfunction), and may not be effective in addressing issues associated with MS symptoms, adverse effects of treatment, or the psychological impact of the disease.
Over the past few years, researchers have increasingly focused on nondrug treatments such as psychological and behavioral interventions. However, so far, there is no clinical standard for assessing or treating sexual dysfunction in the context of MS care, and many health care providers who care for individuals with MS are unsure how to broach this topic.
How did the authors study this issue?
Various nondrug interventions have been used to treat sexual impairment or improve sexual satisfaction, including cognitive behavioral therapy, psychosexual therapy, and group mindfulness-based stress reduction techniques. Researchers from several European countries reviewed six studies about such nondrug treatments of sexual dysfunction in MS, with a total of 295 participants. Two studies included only women and two others included only couples, with average ages ranging from 32 to 47 years. The review, published in 2020 in the International Journal of MS Care, included four studies with interventions targeted directly at treating sexual dysfunction in individuals with MS. The fifth study centered on a mindfulness yoga program designed to improve fatigue and quality of life, and the last study included strategies for improving depression in people with MS.
Are psychological interventions helpful?
Psychobehavioral treatment approaches significantly improved sexual impairment and self-reported sexual satisfaction in all six studies. Although the results were based on a small number of studies, and the reports of improvement in sexual dysfunction were collected over a short period of time (up to 3 months), the review may cause a shift in perspective when it comes to sexual dysfunction and MS care. The authors hoped that the detailed information about various treatment options and their efficacy may help health care providers broach the topic of intimacy during appointments with individuals with MS and offer them some solutions.
The various studied interventions improved sexual impairment and helped to reduce its psychological effects, but it is hard to say which intervention would be ideal for people with MS. The authors recommended using a multidisciplinary model of care, which may involve referrals to psychotherapists and other behavioral health care providers. The review showed that models used in sex therapy may be beneficial for treating sexual impairment in people with MS. Therapies that are tailored to each individual’s or couple’s specific needs are likely to be most beneficial.
Concerns about intimacy and sexuality can affect people’s relationships and quality of life and are likely to increase over time if left untreated. Screening for symptoms of sexual dysfunction during routine appointments should become standard practice for health care providers who treat individuals with MS.
Original Article
Psychobehavioral Treatment Options for Sexual Dysfunction in Multiple Sclerosis: A Systematic Review
International Journal of MS Care
Jana Pöttgen, PhD; Wim van de Vis, MSc (Psych); An van Nunen, MD; Anita Rose, PhD; Jannie Engelbrecht, MSc (Psych); Michelle Pirard, MSc (Psych); Stephanie Lau, MSc (Educ); Christoph Heesen, MD; Sascha Köpke, PhD; Rehabilitation in Multiple Sclerosis (RIMS) Special Interest Group on Psychology and Neuropsychology
Abstract
Background:
Sexual dysfunction in multiple sclerosis (MS) is a significant but overlooked impairment, and treatment options are rare. The aims of this systematic review were to identify psychological interventions used to treat sexual dysfunction in MS, to estimate their benefit, and to note appropriate treatment approaches for research projects and clinical use.
Methods:
A systematic review update was conducted to find psychological interventions aiming to improve sexual dysfunction in MS. A comprehensive search and review of MEDLINE, PsycINFO, CINAHL, and PubMed were completed, and the effects and quality of selected studies were reported.
Results:
Six publications with 295 participants were identified. All selected studies assessed the effectiveness of psychological interventions on sexual dysfunction or sexual satisfaction in people with MS; four studies directly targeted sexual dysfunction in MS, one was a mindfulness yoga program to improve fatigue and quality of life, and one other presented a secondary analysis of a study targeting depression in MS. All six studies reported significant improvements in sexual dysfunction or sexual satisfaction and somewhat in psychological variables.
Conclusions:
A pressing need for development and adequate evaluation of psychological interventions for sexual dysfunction in MS remains. In addition, assessment of sexual dysfunction in MS and its treatment should be more focused in clinical care.
Multiple sclerosis (MS), Psychological intervention, Rehabilitation, Sexual dysfunction, Systematic review
Multiple sclerosis (MS) is a disease of the central nervous system.1 Neurodegeneration and nerve pathway disruption lead to functional impairment in different domains and to the psychological burden of patients. Sexual dysfunction is a hidden disturbance in MS and can be noted to occur in the early stages of the disease.2
No general definition of sexual dysfunction currently exists. Diagnostic classification systems such as the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition)3 and the International Statistical Classification of Diseases, Tenth Revision4 bring different theoretical approaches into a clinically helpful nomenclature. The World Health Organization (WHO) describes human sexuality in general as a broad concept with a variety of experiences and expressions, including thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships.5 They define sexual health as “… a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity.”
Sexual dysfunction is prevalent in 33% to 75% of women and 47% to 75% of men with MS, and age as well as sex differences exist for a variety of primary, secondary, and tertiary sexual dysfunctions.6,7 Particularly, the sexual life of women often suffers in the period shortly after receiving the MS diagnosis.8 In contrast, treatment options for sexual dysfunction in MS are rare and monodimensional (mainly focusing on primary sexual dysfunction).
This review summarizes clinical and behavioral aspects of sexual dysfunction in MS and mainly focuses on recent evidence of psychobehavioral treatment options for sexual dysfunction. It highlights possible treatment options for these frequently overlooked aspects of the disease.
Sexual Dysfunction in MS and Its Treatment
Sexual dysfunctions in MS are subclassified as primary, secondary, and tertiary.9 Primary sexual dysfunction in MS is caused by MS-related neurologic changes in the central nervous system, such as damage in the brain, in the spinal cord areas, and in the peripheral neurons engaged in sexual response.10–12 Female primary sexual dysfunction in MS includes reduced libido (up to 85%), difficulties in achieving orgasm (up to 73%), reduced lubrication (up to 47%), changes in vaginal sensation (up to 30%), and anorgasmia (29%).7 Primary sexual dysfunction in men with MS mainly refers to reduced libido (up to 70%), incomplete or total loss of erectile functions (up to 67%), and inability to ejaculate or premature ejaculation (up to 52%). In their 6-year follow-up study, Kisic-Tepavcevic and colleagues7 found an increase for all observed primary sexual dysfunction in both men and women with MS.
Secondary sexual dysfunction is related to symptoms directly associated with MS or its treatment, eg, fatigue, cognitive decline, pain, neurogenic bowel and bladder problems, or spasticity.13–15 The role of hormone dysregulation in MS is evident,16 but the relation between sexual dysfunction and hormonal status is still unclear. Lombardi et al17 reported no significant correlation between hormonal status and sexual dysfunction in women with MS. Similar results were found for the associations between the degree of disability (measured by the Expanded Disability Status Scale [EDSS]) and sexual function. Winder et al18 reported finding no significant relationship between disability and sexual dysfunction in women with MS, whereas Gumus et al19 showed significant correlations between EDSS score and sexual dysfunction in women with MS. Finally, medications for MS-associated symptoms (eg, amantadine, baclofen, gabapentin, tricyclic antidepressants, and selective serotonin reuptake inhibitors) can negatively affect sexual function.20
Tertiary sexual dysfunction in patients with MS can be caused by personal and psychosocial circumstances and mood disorders related to MS. Recently, we13 reviewed the existing literature regarding sexual dysfunction in MS in relation to neuropsychiatric aspects in MS and found significant correlations between sexual dysfunction and a variety of psychological factors (eg, depression, anxiety, quality of life [QOL], relationship factors, coping abilities).
Despite the clear evidence for sexual dysfunction in MS and its burden for patients, the problem is frequently overlooked in the clinical contact with health care professionals. There may be several reasons for this. It may be due to the heterogeneous nature of sexual dysfunction in MS, with different functional and psychological aspects related to primary, secondary, and tertiary sexual dysfunction21 and with difficulties in investigating specific beneficial effects of interventions. Another reason could be the barriers for people with MS and health care professionals to talk about intimacy and sexual dysfunction. A recent study22 found that the most common barriers reported by patients were the perceived dominance of neurologic symptoms, the presence of family or friends, and not being asked. Barriers reported by health care professionals were the presence of family or friends, lack of knowledge about sexual dysfunction, and inadequate time during the consultation. The authors conclude that the reported barriers could be addressed through modifications in the clinical environment, raising awareness, and providing training opportunities for health care professionals.
Using the same classification of sexual dysfunction in MS, drug treatment can be classified in the context of primary, secondary, and tertiary sexual dysfunction. Medication options for primary and secondary sexual dysfunction in MS, such as sildenafil for men or phosphodiesterase inhibitors for women, have rarely been studied, and results are discordant with a low level of evidence.23 So far, conventional disease-modifying therapies have not been specifically involved in the treatment of sexual dysfunction in MS.24 Recent studies with disease-modifying drugs (natalizumab and interferon beta-1a) found positive and negative effects of MS-related treatment on sexual dysfunction.25,26 Based on the fact that drug treatment is not a panacea for sexual dysfunction in MS,23 the focus of researchers has become increasingly targeted to nonpharmacologic approaches. Nonpharmacologic treatment options comprise psychological and behavioral interventions and approaches focusing on primary, secondary, and tertiary sexual dysfunction in MS.
It could be argued that the treatment of sexual dysfunction in MS should be based on an assessment of sexual dysfunction and should target the specific problem of the patient. As shown in our scoping review,23 sexual dysfunction in MS affects many psychological, neuropsychological, and social life domains. To reduce the burden on patients and their everyday life, psychobehavioral interventions should involve techniques such as compensatory strategies, using aids, supporting the patient’s awareness, and counseling patients and their partners about how to manage their specific sexual dysfunction.
Essential to psychological interventions targeting mood disorders like depression or anxiety are specific modules to decrease stress, enhance self-efficacy and self-esteem, and improve psychological coping skills. Comparable tools should also be used in interventions for sexual dysfunction in MS. In addition, mindfulness-based modules could underpin the effects of those interventions.27
The effects of nonpharmacologic treatment of sexual dysfunction have not been studied in MS as broadly as they have been in other diseases (eg, cancer).28,29 Therefore, we aimed to perform a systematic review as an update of our recent review that assessed neuropsychiatric aspects and psychological treatment,”13 this time focusing only on psychobehavioral treatment aspects. It is crucial to perform this review given that sexual dysfunction is common in people with MS and has a multidimensional effect on patients’ everyday life. This review aimed to select and evaluate the published literature regarding psychobehavioral interventions to treat sexual dysfunction in people with MS and to introduce useful treatment options with concrete information and clinical recommendations.
Methods
A systematic review was conducted based on the existing literature regarding psychological and psychobehavioral interventions to treat sexual dysfunction in people with MS. We searched PubMed, MEDLINE, CINAHL (Cumulated Index to Nursing and Allied Health Literature), and PsycINFO for the following terms: multiple sclerosis, sex, sexual disorders, sexual symptoms, lubrication, orgasm, and sexual satisfaction. In addition, we hand-searched the reference lists of articles we found using the same criteria. Studies were limited to those written in English or German. Only studies that used psychobehavioral interventions with more than ten participants were included. Psychobehavioral interventions were defined as interventions that used any type of psychological or psychobehavioral methods (eg, cognitive behavioral therapy [CBT], mindfulness therapy, mixed psychological approaches) to deal with MS-related impairment. Further inclusion criteria were any sexual dysfunction or sexual behavior as a primary or secondary outcome measure. In addition, we included only studies that assessed sexual dysfunction at least at the preintervention and postintervention time points. Interventions did not have to target sexual dysfunction in MS.
We used relevant studies included in a previous review on sexual dysfunction13 that had applied a similar search strategy but was not restricted to intervention studies and had included studies published before November 2016. Therefore, the present search was restricted to studies published since November 2016. The latest search was conducted on December 31, 2019. Titles retrieved by the search were screened by two of four independent reviewers (J.P., W.v.d.V., A.v.N., S.L.), and discrepancies were discussed and resolved. Reviewers were not blinded to study authors. The following data were extracted using a standardized data extraction form: 1) sample size, 2) demographic features of participants, 3) type and duration of intervention (number of weeks, number of hours per week), 4) type of control group, 5) primary and secondary outcomes, 6) duration of follow-up data collection, and 7) baseline, postintervention, and, if applicable, follow-up data.
Study Quality Assessment
We used the appropriate Critical Appraisal Skills Programme (CASP) tools to determine the validity and quality of the studies.30 CASP checklists have been developed for reviews of randomized controlled trials (RCTs), systematic reviews, qualitative, case-control, diagnostic, cohort, economic designs, and clinical prediction rule. Scores range from 0 to 7, with higher values indicating better quality.
Two reviewers (J.P., S.K.) assessed the studies separately according to CASP tool requirements and discussed and resolved discrepancies in their assessments.
Results
Study Selection
The updated search identified 145 publications, of which 140 were excluded by title screening because no psychobehavioral interventions in relation to sexual dysfunction in MS were conducted in the studies. One of the five selected studies was excluded because it was based on a single case design, and another was excluded because it was a review itself regarding treatment for sexual dysfunction in MS. The remaining three publications were selected for full-text screening.31–33
After reading full-text articles, all three publications met the inclusion criteria and were included. We added three intervention studies,34–36 identified in our former review,13 resulting in six studies included in the present review (Figure S1, published in the online version of this article at ijmsc.org).
Study Characteristics
Four of the six included studies were RCTs,31–33,36 two used an observational longitudinal pre-post assessment design,34,35 and all were published in English (Table 1). Three of the interventions targeted sexual dysfunction in MS directly,32,35,36 and one study used a specific sexual therapy but mainly focused on improvement in QOL.33 One was a depression treatment study using a secondary analysis of the results from the whole study group regarding sexuality in MS.34 One study targeted fatigue reduction, with a secondary outcome measure for satisfaction of sexual dysfunction in MS.31 Group sessions were used in two of the studies,31,33 one study used a telephone-administered CBT intervention,34 and another was delivered with personal contact sessions with a licensed clinical psychologist for the experimental group (the couple came to two in-person 2-hour sessions).32 One study was delivered face-to-face in a one-on-one session design,36 and another did not specify the delivery method with clarity.35
Table 1
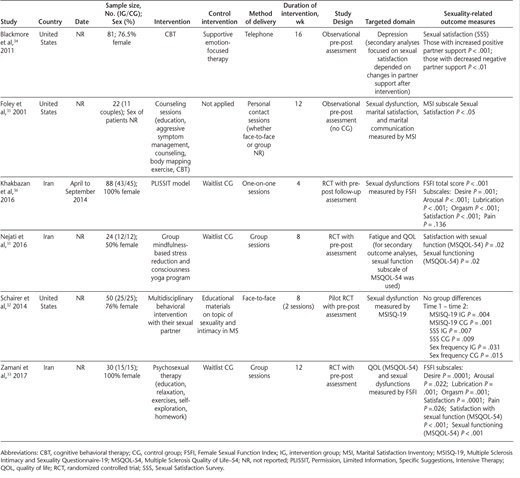
Intervention duration was 4 to 16 weeks; five studies used a pre-post assessment design, and only one study reported an additional follow-up assessment 2 to 3 months after the intervention.36
Control groups received usual care (n = 3),31,33,36 supportive emotion-focused therapy (n = 1),34 or educational materials on the topic of sexuality and intimacy in MS given by a doctoral graduate student (n = 1)32 ; one study did not recruit a control group.35 Trials were performed in the United States (n = 3) and Iran (n = 3).
Participants
The number of study participants was small, ranging from 22 to 88, with a total of 295 participants. In two studies, only women participated,33,36 and two others included only couples.35,37 The mean age of participants ranged from 32.1 to 47.7 years, and the mean years since disease onset was reported for three studies and ranged from 3.7 to 10.3 years.
Interventions
Four approaches directly targeted sexual dysfunction: one used counseling sessions, with different lessons on education, aggressive symptom management, counseling, body mapping exercise, and CBT35 ; one used the Permission, Limited Information, Specific Suggestions, Intensive Therapy (PLISSIT) model36 ; and one used a brief two-visit multidisciplinary behavioral intervention using a consultation model.32 Another approach used psychosexual therapy with educational lessons, relaxation, exercises, self-exploration, and homework.33 One intervention used CBT mainly targeting depression reduction.34 Another intervention was a group mindfulness-based stress reduction and consciousness yoga program that mainly targeted benefits related to fatigue and QOL.31
Outcomes and Time Points
Studies used different measures for sexual function, with the Female Sexual Function Index (FSFI) used in two studies.33,36 The sexual function subscale of the Multiple Sclerosis Quality of Life–54 (MSQOL-54) was also used in two studies.31,33 Two studies used the Sexual Satisfaction Survey,32,34 and the Sexual Disabilities section of Guy’s Neurological Disability Scale was used in one study.34 Another study applied the Marital Satisfaction Inventory.35 The Multiple Sclerosis Intimacy and Sexuality Questionnaire-19 was also used in one study.32
Further psychological outcome measures were the Beck Depression Inventory, used to measure depression in two studies34,36 ; the Fatigue Severity Scale, used to assess fatigue in two studies31,36 ; and the MSQOL-54, used to evaluate QOL in three studies.31,32,33 To measure social support, the University of California at Los Angeles Social Support Scale was used in one study.34 To measure marital adjustment, the Locke-Wallace Marital Adjustment Test was used in one study.35
The Structured Clinical Interview for DSM-IV was used to assess psychiatric diagnoses, and the Marital Satisfaction Inventory affective communication and problem-solving communication scales were used to measure intimate communication in two studies.31,35
In five of the six studies, all outcomes were reported at baseline and directly after the intervention.31,33–36 One study used the 4 weeks after the last intervention for the postassessment to give the participants enough time for homework and adaption.32 Only one study reported follow-up data for 2 and 3 months after the intervention.36 For neurologic assessment, three studies used the EDSS,32,35,36 and the Minimal Record of Disability for MS was used in one study.35
Study Quality Assessment
Results of the CASP assessments are shown in Table S1. Quality ratings for the interventional studies ranged from 2 to 6 of 7. Heterogeneity in sampling, data collection, and measurement of identified variables was noted between studies.
Screening of patients before inclusion was applied in all the studies. Randomization was conducted in four of six studies, one study was a second observational analysis of all participants.34 One was a single-arm observational study.35 Three of the six studies reported a quasi-experimental design.31,33,35 No trial was stopped before the finish, and only two studies clearly reported the analytic process (participants were analyzed by the group to which they were assigned ).32,36 Blinding of all participants and clinical staff (health care workers and study personnel) was not realized in any of the trials. In five of the six trials, the groups were comparable before the intervention started.31–34,36 In four trials, the groups were treated equally aside from the experimental design.31–34 Only one trial clearly specified the primary outcome in an appropriated way,32 and again only one study reported confidence intervals for the results32 ; no other quality calculations were reported in any other study.
Synthesis of Results
Four of six studies reported group differences with beneficial effects of psychobehavioral interventions on sexual dysfunction.31,33,34,36 One other found a significant improvement in both the intervention group and the control group receiving only informational material regarding sexual dysfunction in MS.32
Another study, which did not include a control group, found significant beneficial effects of the treatment between preassessment and postassessment.35 Different aspects of sexual dysfunction were observed, including sexual satisfaction and sexual functioning. Studies that directly targeted sexual dysfunction32,33,35,36 showed larger improvements compared with those that focused on the treatment of other psychological domains, such as QOL, fatigue,31 and depression.34
Discussion
Sexual dysfunction and the involved psychological risks have been well studied in people with MS.13 Sexual problems can occur at any point of the disease and in all disease courses. Strong associations with increased depression, anxiety, and fatigue; reduced QOL; and negative effect on relationship have been described. Implications related to fertility, pregnancy, and parenting are unknown but seem likely. Therefore, regular screening for sexual dysfunction seems warranted in people with MS, including a detailed evaluation and specific assessment of underlying causes when there seems to be a problem with intimacy and/or sexuality. Unfortunately, the standard clinical assessment mostly ignores this important factor of disease burden.22 Also, many barriers—such as focusing on supposedly more important neurologic symptoms, sense of shame, and clinicians’ lack of knowledge, consultation time, but also treatment options—play important roles in sexual dysfunction in MS being ignored. In addition, individuals with physical disabilities, which are frequent in MS patients, have been shown to have a negative attitude regarding their body.38 This may lead a person with MS to feel less attractive and to hide personal needs of sexual expression.
In contrast to the known prevalence of sexual dysfunction in MS, treatment options particularly for secondary and tertiary sexual dysfunction are rare, and drug treatment options for primary sexual dysfunction are not convincingly effective.23 This updated systematic review included six studies and showed beneficial effects of psychobehavioral treatment approaches for sexual impairment and sexual satisfaction in people with MS. Unfortunately, the small number of intervention studies limits the interpretation of results, but, based on the findings of this review, psychobehavioral interventions seem to be effective in decreasing patient-reported sexual dysfunction in the short term (and up to 3 months). According to the CASP assessment (Table S1), the quality of evidence has to be considered weak, and publication bias seems highly likely considering the small sample size of included studies. In addition, many different domains were targeted and, because different outcome measures were used, led to important challenges for a stringent and meaningful synthesis of the data. Due to the obviously marked heterogeneity and because of the small number of included trials, we decided to present outcome data narratively without conducting statistical analyses or meta-analyses. The included trials do not support a decision as to which of the interventions would be most effective in treating sexual dysfunction in MS. Therefore, we are unable to recommend a preferable type of intervention. However, it indicates that interdisciplinary care should be considered for holistic rehabilitation approaches to treat sexual dysfunction in MS from a holistic rehabilitation perspective.
Therefore, more research is clearly needed. Specifically, the development and validation of assessment tools for sexual dysfunction in MS should be the focus of future research activities. The present review provides several implications for future research in the treatment of sexual dysfunction in MS. Given that the evidence from many studies indicates that sexual dysfunction in MS worsens over time,7 larger RCTs with treatment approaches for sexual dysfunction in MS should be the focus of research. Instead of merely applying usual care, control interventions should be comparable with interventions concerning effort and attention. In addition, it could be important to include partners of patients. Finally, sexual dysfunction outcomes examined in studies should include both sexual functioning and sexual satisfaction.
Despite the limited evidence presented in this review, the information presented can provide health care providers with detailed information about treatment approaches and may help them to better discuss with patients this intimate part of life. In addition, the PLIS-SIT model could be named as a complex intervention39 with potential treatment effects. The intervention combines a comprehensive behavioral approach with a standardized and structured treatment plan and was successful in different neurologic and other conditions (stroke, spinal cord injury, breast cancer) and currently seems to be the most successful program to treat sexual dysfunction in general as well as in specific diseases. Treatment descriptions of the PLISSIT model can be found in many publications (eg, Mercer40 ). A standardized user guide for practice use also exists.41
The relationship between sexual dysfunction in MS and neuropsychiatric impairment (eg, cognition, depression, fatigue), and their common effect on social relations, is multifactorial and complex. The extent to which they are consequences of the disease process itself or secondary psychological responses remains unclear. However, both assessment and treatment of sexual dysfunction in MS should become clinical standard. Because sexual dysfunction in MS varies between patients/couples, all participants should receive the combination of therapy that is adjusted to individual needs.
This review has limitations. Due to the small number of available studies, we were unable to conduct meaningful subgroup analyses, although we included all studies irrespective of study design (RCT, observational study) and content (targeting sexual dysfunction in MS or other domains, such as fatigue or QOL). Also, the study target groups differ (singles, couples). This may confound the results of the present review. In addition, analyses were performed on self-reported data. This is useful because sexuality is a very personal issue. Nevertheless, the validity of effects may be overestimated due to lack of blinding. Finally, only one study provided information on long-term effects.
In summary, it seems clear that concerns about intimacy and/or sexuality in MS are likely to increase when left untreated. Although the present review provides only weak evidence for the benefit of psychological treatment of sexual dysfunction, it highlights the need for regular screening for sexual dysfunction in patients with MS and referral of affected patients for professional help. The present results imply directions for future research and the need for changes in clinical practice, which may lead to optimized care and consequently improved QOL for people with MS. Because previous research indicates a strong association between sexual dysfunction in people with MS and psychological and social functioning, potential interventions for the treatment of sexual dysfunction in MS, such as the PLISSIT model, should be addressed in further research.
PRACTICE POINTS
A systematic literature review of psychological interventions for sexual dysfunction in MS identified only six articles published between November 2016 and December 2019.
In these six studies, four interventions targeted sexual dysfunction directly and one each focused on depression and mindfulness-based stress reduction.
Positive results were reported in all the studies, although methodological limitations affected the strength of the evidence.
The RIMS (Rehabilitation in MS; www.eurims.org) Special Interest Group on Psychology and Neuropsychology: Belgium—National MS Centre Melsbroek: M. Pirard; Denmark—Sclerose Hospital Erne, Ry: J. Engelbrecht; Finland—Neurological Masku Rehabilitation Centre, Masku: P. Hämäläinen; Germany—Institute for Neuroimmunology and MS Research, University Medical Center Hamburg-Eppendorf, Hamburg: J. Pöttgen, S. Lau; the Netherlands—Ziekenhuis Groep Twente, Hengelo: W. van de Vis; Slovenia—University Medical Centre, Ljubljana: A. Ozura; Spain—CemCat Hospital Vall d’Hebron, Barcelona: C. Cerqueda; United Kingdom—South Newton Hospital, Salisbury: A. Rose.
