Prevalence of Posttraumatic Stress Disorder in Patients with Multiple Sclerosis
Why is this article of interest to me?
We typically associate posttraumatic stress disorder (PTSD) with combat veterans and individuals who have experienced a traumatic event. Researchers estimate that about 6.8% of the general population suffers from PTSD. Although we tend not to associate disease with PTSD, we agree that both acute and chronic disease inflicts considerable stress on people and can affect their relationships with family, friends, and co-workers. This brief article seeks to define and measure the incidence of PTSD among a group of individuals who have MS.
How was this study conducted?
The investigators screened 988 individuals who had been diagnosed with RRMS, progressive MS, or secondary progressive MS and assessed them for PTSD using the criteria outline in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR). Of these individuals, 76.8% were female with a mean age of 41.2 years. Using the DSM-IV-TR criteria, they identified 56 who met the diagnostic measures of PTSD. The mean age of these individuals was 40.8 years, and 83.9% were female.
What did this study show?
This particular study demonstrated that the prevalence of PTSD among this group of individuals with MS was about 5.7%, somewhat less than the estimated prevalence among the general population. This percentage, however, masks the significant number (21.4%) of individuals who declined to participate in the screening or chose to leave the study. After accounting for these individuals, the investigators estimate the actual prevalence of PTSD among these individuals to be approximately 8.5%.
What is my take-away from this article?
Having MS or any other disease does not in itself qualify as the factor that causes PTSD — there are very specific DSM-IV-TR criteria in a diagnosis of PTSD. Regardless of whether you believe that you suffer from PTSD, this article can help you to reflect on how MS may create stress for you and, above all, to communicate these feelings to your healthcare provider.
We associate PTSD with a traumatic event that took place in the near or distant past. Yet stress for many individuals with MS looks both forward and backward: an event such as paralysis or incontinence can remain traumatic long after it has resolved, while fear of relapse or disease progression in the future weighs heavily on the thoughts of many people.
The investigators in this study agree that more data are required before we understand how common PTSD may be among people with MS. For most individuals, this article serves as a reminder to recognize when stress may become difficult to manage and to reach out for help to your healthcare provider.
Original Article
Prevalence of Posttraumatic Stress Disorder in Patients With Multiple Sclerosis
Sara Carletto, PhD, Martina Borghi, PsyD, Francesco Scavelli, MSc, Diana Francone, PsyD, Maria Luisa Perucchini, MSc, Marco Cavallo, PhD, Francesco Pagnini, PhD, Antonio Bertolotto, MD, Francesco Oliva, MD, and Luca Ostacoli, MD
The Journal of Nervous and Mental Disease
Abstract
Chronic and life-threatening illnesses, such as multiple sclerosis (MS), have been identified as significant stressors potentially triggering posttraumatic stress disorder (PTSD). The study aims to investigate the prevalence of PTSD according to Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria in a large sample of patients with MS. A total of 988 patients with MS were screened with the Impact of Event Scale–Revised, and then assessed with the PTSD module of the Structured Clinical Interview for DSM-IVand with the Clinician-Administered PTSD Scale to confirm PTSD diagnosis. Posttraumatic symptoms were reported by 25.5% of the sample. A confirmed diagnosis of PTSD was found in 5.7% of patients, but prevalence could reach 8.5%, including also dropout patients. Further studies are needed to evaluate if adjustment disorder could better encompass the frequently encountered subthreshold posttraumatic stress symptoms and how clinicians can deal with these symptoms with appropriate interventions.
According to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association [APA], 2000), posttraumatic stress disorder (PTSD) is a clinical condition developed after exposure to a traumatic event. Symptoms include intense fear, helplessness, or horror; persistent reexperiencing of the traumatic event; persistent avoidance of stimuli associated with the event; and increased arousal. The prevalence of PTSD in the general population according to DSM-IV criteria was 6.8% (Kessler et al., 2005).
Chronic and potentially life-threatening illnesses were explicitly included in DSM-IV as a stressor that could precipitate PTSD (APA, 2000). Since then, there has been empirical evidence of high rates of PTSD in patients affected by various life-threatening illnesses, including myocardial infarction, cancer, intensive care treatment, HIV, and other medical conditions (Chalfant et al., 2004; Kangas et al., 2002; Tedstone and Tarrier, 2003). Patients with a medical disease, however, are rarely screened routinely for PTSD symptoms despite its long-lasting impact on relational, social, and working functioning, which may also lead to a poor compliance (Tedstone and Tarrier, 2003)
Posttraumatic stress reactions in medical illnesses present significant peculiarities: it may be difficult to identify a single traumatic stressor that may persist over time and eventually worsen in cases of disease progression; the stressor is typically ongoing and future oriented (e.g., fear of relapsing episodes, fear of the progression of the disease); the criterion of reexperiencing the threatening event is associated with the risk of reoccurrence of the symptoms (Chalfant et al., 2004; Kangas et al., 2002; Tedstone and Tarrier, 2003).
Multiple sclerosis (MS) is an inflammatory disease of the central nervous system that affects both the brain and the spinal cord. MS is characterized by significant motor impairment and additional neuropsychiatric and cognitive symptoms. For many patients, MS diagnosis itself can be considered as a trauma (Chalfant et al., 2004; Counsell et al., 2013). Furthermore, in addition to the psychological consequences of the diagnosis and treatment of the disease itself, specific events such as an acute episode of paralysis of both legs, or urge incontinence in a public context may represent a real traumatic event for patients with MS.
To date, there are few studies evaluating the prevalence and the characteristics of PTSD related to MS. Counsell et al. (2013) found that almost 55.1% (n = 69/126) of a MS sample recruited through the Internet reported that having MS was at least somewhat traumatic, although they did not explicitly investigate for PTSD criteria. In another study, Chalfant et al. (2004) evaluated a small sample of patients with MS, observing a relatively high rate of patients with PTSD (n = 9/58, 15.5%). However, in a previous study by our research group (Ostacoli et al., 2013), we found a significantly lower prevalence of PTSD (12/232, 5.2%) than those reported by Chalfant et al. (2004).
The aim of the current study was to further investigate the prevalence of traumatic stress and PTSD related to the diagnosis in a larger sample of persons with MS with a structured methodology.
Methods
A total of 988 patients with MS were consecutively recruited from 2010 to 2013 at the Regional Reference Centre for Multiple Sclerosis (CReSM) affiliated with the University Hospital “San Luigi Gonzaga” of Orbassano, Turin, Italy, which served about 1500 patients with MS coming from Piedmont and neighboring regions.
This study was approved by the Research Ethics Committee of the University Hospital San Luigi Gonzaga (protocol number 14/2010). Informed consent was obtained from all the participants
The inclusion criteria of the study were a definite diagnosis of a relapsing-remitting, primary or secondary progressive MS disease according to the standard international criteria (Polman et al., 2011), received at least 6 months before our evaluation.
All the consecutive patients with MS that presented themselves at the CReSM for a routine visit, a blood test, or an infusion therapy were invited to participate in the study and completed the Impact of Event Scale–Revised (IES-R; Weiss and Marmar, 1997), a 22-item self-report measure with a high internal consistency (α = .96; Creamer et al., 2003), that assesses distress caused by traumatic events. Patients were instructed to complete this questionnaire referring only to MS as the traumatic event.
Patients with scores equal or above the cut-off of 33 were assessed with the PTSD module of the Structured Clinical Interview for DSM-IV (SCID; First, 1997) to confirm PTSD diagnosis. Finally, patients with a positive diagnosis of PTSD were also assessed with the ClinicianAdministered PTSD Scale (CAPS; Blake et al., 1995), a clinical semistructured interview based on DSM-IV-TR and considered the “gold standard” assessment tool for PTSD. This scale has excellent support for its reliability, with alpha coefficients ranging from .64 to .88 (Weathers et al., 2001).
All the instruments were administered by two clinical psychologists with experience in the liaison setting, working at the Clinical Psychology and Psychosomatics Service, Mental Health Department of the University Hospital San Luigi Gonzaga
Data were collected and processed by means of Microsoft Office Excel software (2007).
Results
A total of 988 patients with MS completed the screening with the IES-R. Of these 988 patients, 759 (76.8%) were female, and the mean age was 41.2 (SD = 10.53).
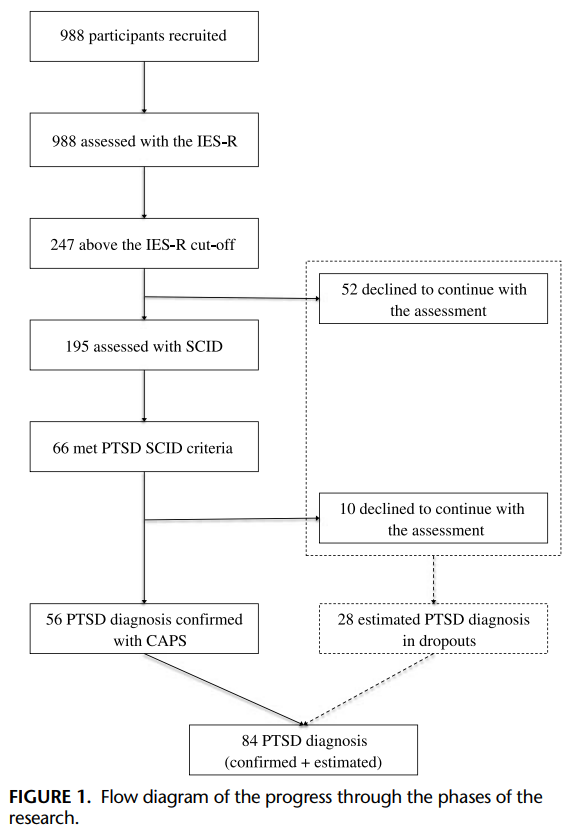
Two hundred forty-seven (25%) of 988 patients presented an IES-R score above the cutoff, suggesting the possible presence of PTSD. Fifty-two (5.3%) patients refused to continue the evaluation (refusal rate, 21.1%). Of the other 195 patients, 66 patients met the criteria of PTSD diagnosis according to the SCID criteria (6.7%). CAPS administrations confirmed the SCID evaluations, although 10 (15.2%) patients refused to be assessed with the CAPS.
Therefore, 56 (5.7%) patients were diagnosed with PTSD according to all the diagnostic measures used (i.e., IES-R, SCID, and CAPS). Of these 56 patients, 47 (83.9%) were women and the mean age was 40.8 (SD = 11.12). Refusal to participate in further assessment was relatively high and mostly due to difficulties in reaching the CReSM center.
The prevalence of PTSD as assessed above was 5.7% (56/988). However, this rate could not be verified for those patients with PTSD who had dropped out from the study. On the opposite extreme, if all those who dropped out after the IES-R administration had experienced PTSD, the prevalence would reach 11.94%. In order to try to best account for dropouts, we assumed that those above the IES threshold who dropped out had a similar PTSD prevalence as those who remained in the study (34%) and that SCID outcomes were all confirmed by the CAPS assessment. With this imputation, the expected number of patients who can meet the criteria for PTSD is 84, with an estimated prevalence of 8.5% (Fig. 1).
Discussion
This study explored the presence of PTSD in a large sample of patients with MS. The PTSD prevalence found in our study is in line with the general population (Kessler et al., 2005) and lower than that previously reported among patients with MS (Chalfant et al., 2004). This discrepancy could be explained by methodological differences as Chalfant et al. (2004) only considered a CAPS phone interview, whereas in the present study, we opted for a multistep assessment strategy, comprising the IES-R as first screening, then SCID and CAPS in-person interviews to confirm the PTSD diagnosis and to deepen symptoms evaluation. Furthermore, another strength of the present study is that it referred to a larger population than the previous ones, leading to a more reliable estimation of the actual prevalence rate of PTSD related to MS.
Although it is not possible to predict whether people with PTSD are more or less prone to dropout, the study conducted by Szafranski et al. (2017) suggests that PTSD severity had a limited effect to predict treatment dropout. Therefore, our estimation of 8.5% could slightly underestimate the presence of PTSD. However, this calculation can only be considered as an attempt to deal with the dropout rate, that otherwise can be considered as a limitation of this study. Future studies should reduce as much as possible the number of dropouts in order to reach a more accurate and generalizable estimation of PTSD prevalence in the MS population.
Apart from PTSD diagnosis, we found that 25% of patients with MS presented posttraumatic stress symptoms. In line with previous literature, we can hypothesize that some of these patients could be considered as having subthreshold PTSD, which can be defined as experiencing clinically significant symptoms of PTSD but not meeting full diagnostic criteria for the disorder (Cukor et al., 2010; McLaughlin et al., 2015; Weiss et al., 1992). Several studies showed that patients with subthreshold PTSD display significant impairment in mental and physical functioning, which is comparable to the impairment associated with full PTSD (Grubaugh et al., 2005; McLaughlin et al., 2015; Mota et al., 2016; Zlotnick et al., 2002).
At the same time, a recent study on patients with cancer (Kangas, 2013) highlighted that for patients not meeting the full PTSD diagnostic criteria, but with significant symptoms and/or functional impairment, adjustment disorder (AD) should be considered as a possible alternative.
Moreover, after the beginning of the current study, DSM-5 stated that medical disease per se can no longer be considered as a stressor event that qualifies for a diagnostic criterion in PTSD diagnosis and patients who do not exhibit the full symptom profile of PTSD should be diagnosed as AD (APA, 2013). Therefore, it is possible to suggest that some patients reporting posttraumatic symptoms without fulfilling all PTSD diagnostic criteria could be better recognized as ADs with posttaumatic symptoms.
The main limitation of this study is the lack of data, except for IES-R, sex, and age, about patients with MS who do not present posttaumatic symptoms or PTSD. For this reason, it was not possible to make a comparison between different groups to better categorize the clinical features presented by different subgroups of patients. Furthermore, another major limit is that AD was not specifically investigated; thus, it is not possible to assess whether the symptoms reported by patients with MS, which did not meet a full PTSD diagnosis, may otherwise fall into this diagnostic category.
Future studies should better investigate the prevalence of ADs, discerning between subthreshold PTSD and AD in patients with MS. Nevertheless, these symptoms have an important impact on healthrelated quality of life and patients' functioning (Kapfhammer et al., 2004; Meeske et al., 2001; Rapaport et al., 2005), with an increase also in health care utilization (Tedstone and Tarrier, 2003). It is therefore imperative that these symptoms can be detected by the health care staff and properly addressed with effective treatments.
Previous findings have already supported the efficacy of specific treatment for PTSD in patients with MS (Carletto et al., 2016). Future studies are needed to evaluate if these interventions could be effective also for patients with MS with AD, which according to DSM-5 is more prevalent than PTSD.
In conclusion, this brief report highlights a noteworthy rate of posttaumatic symptoms in patients with MS, which sometimes fulfills the criteria for a PTSD diagnosis. The identification of these symptoms and the application of effective treatments are warranted from a clinical perspective. Further studies are required to better explore how these symptoms develop in time and how they could be addressed by some kinds of intervention.
References
American Psychiatric Association (Ed) (2000) Diagnostic and statistical manual of mental disorders, fourth edition, revised: DSM-IV-TR®. Washington, DC: American Psychiatric Pub.
American Psychiatric Association (Ed) (2013) Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Pub Incorporated.
Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Gusman FD, Charney DS, Keane TM (1995) The development of a Clinician-Administered PTSD Scale. J Trauma Stress. 8:75–90.
Carletto S, Borghi M, Bertino G, Oliva F, Cavallo M, Hofmann A, Zennaro A, Malucchi S, Ostacoli L (2016) Treating post-traumatic stress disorder in patients with multiple sclerosis: A randomized controlled trial comparing the efficacy of eye movement desensitization and reprocessing and relaxation therapy. Front Psychol. 7:526.
Chalfant AM, Bryant RA, Fulcher G (2004) Posttraumatic stress disorder following diagnosis of multiple sclerosis. J Trauma Stress. 17:423–428.
Counsell A, Hadjistavropoulos HD, Kehler MD, Asmundson GJG (2013) Posttraumatic stress disorder symptoms in individuals with multiple sclerosis. Psychol Trauma Theory Res Pract Policy. 5:448–452.
Creamer M, Bell R, Failla S (2003) Psychometric properties of the Impact of Event Scale—Revised. Behav Res Ther. 41:1489–1496.
Cukor J, Olden M, Lee F, Difede J (2010) Evidence-based treatments for PTSD, new directions, and special challenges. Ann N Y Acad Sci. 1208:82–89.
First MB (Ed) (1997) User's guide for the Structured clinical interview for DSM-IV axis I disorders SCID-I: Clinician version. Washington, DC: American Psychiatric Press.
Grubaugh AL, Magruder KM, Waldrop AE, Elhai JD, Knapp RG, Frueh BC (2005) Subthreshold PTSD in primary care: Prevalence, psychiatric disorders, healthcare use, and functional status. J Nerv Ment Dis. 193:658–664.
Kangas M (2013) DSM-5 trauma and stress-related disorders: Implications for screening for cancer-related stress. Front Psychiatry. 4:122.
Kangas M, Henry JL, Bryant RA (2002) Posttraumatic stress disorder following cancer. A conceptual and empirical review. Clin Psychol Rev. 22:499–524.
Kapfhammer HP, Rothenhäusler HB, Krauseneck T, Stoll C, Schelling G (2004) Posttraumatic stress disorder and health-related quality of life in long-term survivors of acute respiratory distress syndrome. Am J Psychiatry. 161:45–52.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 62:593–602.
McLaughlin KA, Koenen KC, Friedman MJ, Ruscio AM, Karam EG, Shahly V, Stein DJ, Hill ED, Petukhova M, Alonso J, Andrade LH, Angermeyer MC, Borges G, de Girolamo G, de Graaf R, Demyttenaere K, Florescu SE, Mladenova M, PosadaVilla J, Scott KM, Takeshima T, Kessler RC (2015) Subthreshold posttraumatic stress disorder in the world health organization world mental health surveys. Biol Psychiatry. 77:375–384.
Meeske KA, Ruccione K, Globe DR, Stuber ML (2001) Posttraumatic stress, quality of life, and psychological distress in young adult survivors of childhood cancer. Oncol Nurs Forum. 28:481–489.
Mota NP, Tsai J, Sareen J, Marx BP, Wisco BE, Harpaz-Rotem I, Southwick SM, Krystal JH, Pietrzak RH (2016) High burden of subthreshold DSM-5 posttraumatic stress disorder in U.S. military veterans. World Psychiatry. 15:185–186.
Ostacoli L, Carletto S, Borghi M, Cavallo M, Rocci E, Zuffranieri M, Malucchi S, Bertolotto A, Zennaro A, Furlan PM, Picci RL (2013) Prevalence and significant determinants of post-traumatic stress disorder in a large sample of patients with multiple sclerosis. J Clin Psychol Med Settings. 20:240–246.
Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, Fujihara K, Havrdova E, Hutchinson M, Kappos L, Lublin FD, Montalban X, O'Connor P, Sandberg-Wollheim M, Thompson AJ, Waubant E, Weinshenker B, Wolinsky JS (2011) Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 69:292–302.
Rapaport MH, Clary C, Fayyad R, Endicott J (2005) Quality-of-life impairment in depressive and anxiety disorders. Am J Psychiatry. 162:1171–1178.
Szafranski DD, Snead A, Allan NP, Gros DF, Killeen T, Flanagan J, Pericot-Valverde I, Back SE (2017) Integrated, exposure-based treatment for PTSD and comorbid substance use disorders: Predictors of treatment dropout. Addict Behav. 73:30–35.
Tedstone JE, Tarrier N (2003) Posttraumatic stress disorder following medical illness and treatment. Clin Psychol Rev. 23:409–448.
Weathers FW, Keane TM, Davidson JR (2001) Clinician-Administered PTSD Scale: A review of the first ten years of research. Depress Anxiety. 13:132–156.
Weiss DS, Marmar CR (1997) The Impact of Event Scale–Revised. In Wilson JP, Keane TM (Eds), Assessing psychological trauma and PTSD. Assessing Psychological Trauma and PTSD (pp 399–411). New York, NY: Guilford Press.
Weiss DS, Marmar CR, Schlenger WE, Fairbank JA, Kathleen Jordan B, Hough RL, Kulka RA (1992) The prevalence of lifetime and partial post-traumatic stress disorder in Vietnam theater veterans. J Trauma Stress. 5:365–376.
Zlotnick C, Franklin CL, Zimmerman M (2002) Does “subthreshold” posttraumatic stress disorder have any clinical relevance? Compr Psychiatry. 43:413–419.