Effectiveness of Aquatic Therapy for Individuals With Multiple Sclerosis: A Systematic Review
- Why is this important?
In order to decrease the progressive effects of MS, physical therapists may take different approaches, and Aquatic therapy is one recommended intervention for individuals with MS. The natural buoyancy and viscosity of water can potentially provide a safe and protective environment for individuals with MS to undertake exercise by making it easier to move without the fear of falling .The cooling effect of 85°F water, the temperature of a typical swimming pool (10-12°F cooler than human body temperature), also makes it possible to be active without overheating. Additionally, these activities do not require a highly competent swimming technique to reap the benefits.
- How did the authors study this issue
Studies were conducted in 2019 on 8 different articles with aquatic therapy as their primary subject of study. A 10-point scale was used to score articles on validity and statistical information: scores of 9 or 10 are considered excellent, 6-8 are good, 4 or 5 are fair. Five of them were categorized as good and three as fair, with a total of 305 subjects living with MS included in the analyses.
- What did the study show?
The most common benefit throughout each study was the improvement on fatigue. The subjects participated in aquatic therapy for extended period of times (8 to 20 weeks), showing decrease in fatigue severity. One of the studies did not show fatigue-related improvements, however the duration or frequency of this program (3 weeks) may have not been enough to show significant improvement.
Balance was also addressed in two of the eight controlled trials, and in both studies there was a significant improvement among the aquatic exercise group compared with baseline.
The studies also examined depression, and subjects were in the no/minimal or mild depression categories following the program. Compared with a non-exercise condition, both yoga and aquatic exercising three times a week for eight consecutive weeks positively influenced fatigue, depression, and paresthesia in female patients with MS.
Three studies also measured significant improvements in Quality of Life, with each study presenting slightly different types of exercise, frequency, and duration.
Pain reduction was measured comparing 2 different groups: the first was engaged in a Ai- Chi exercise program in which the subjects performed slow, relaxing big movements in a pool at shoulder depth, the second group in this trial performed the same relaxation exercises as the aquatic group but did not get the Ai-Chi interventions in the pool. The subjects who performed aquatic exercises showed significant reduction in pain perception.
Walking ability, which also impacts Quality of Life, showed improvements: aquatic exercise resulted in a higher average walking speed over 500 m, of about 7.6% proving that aquatic therapy can be an effective intervention for improving household and community ambulation in people with symptoms of MS.
Overall, the evidence supports that aquatic therapy is beneficial for individuals with MS improving fatigue, pain, depression, balance, walking ability and Quality of Life.
For any questions, please make sure to contact your Healthcare Provider.
Original Article
Effectiveness of Aquatic Therapy for Individuals With Multiple Sclerosis: A Systematic Review
Journal of Aquatic Physical Therapy
Schoeneberg, Becky PT, DPT; Arcadipane, Nicolas PT, DPT; Bussa, Brandon PT, DPT; Haselwood, Emily PT, DPT
Abstract
Background and purpose.
Multiple sclerosis (MS) is an inflammatory, demyelinating disease that attacks the central nervous system. It is estimated that from 350,000 to 400,000 people in the United States are affected by MS. This study is a systematic review of randomized controlled trials (RCTs) evaluating the benefits of aquatic therapy for people with MS.
Methods.
Databases used in this study were Academic Search Premier, Academic Search Elite, CINAHL Complete, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, MEDLINE, MEDLINE with Full Text, SPORTDiscus with Full Text, and Cochrane Clinical Answer. RCTs included in this systematic review were analyzed using the PEDro scale.
Results.
After the primary investigators independently screened 1,019 articles, eight RCTs were included in the systematic review. The average PEDro score was 5.875, with a range of 4 (fair) to 7 (good). Various outcome measures were used to quantify benefits of aquatic therapy for the MS population.
Discussion and conclusions.
Aquatic therapy is beneficial for individuals with MS. These benefits include, but are not limited to, significant improvement in fatigue, quality of life, pain, balance, walking ability, and depression.
Introduction
Multiple sclerosis (MS) is an inflammatory, demyelinating condition that affects the central nervous system. Sclerotic plaques form after an exacerbation in the brain, brainstem, and spinal cord. An estimated 350,000-400,000 individuals in the United States are affected by MS.1 Additionally, 50% of these individuals will need some sort of assistance with walking within 15 years of the disease onset.2 MS presentation varies depending on the location of the plaques. Fatigue is one of the many symptoms of MS, but it is the most common symptom occurring in 65%-97% of patients.1 Demyelination in association with axonal damage leads to the slowing or blockage of nerve signals. This blockage can result in other common MS symptoms such as visual problems; pain; sensations of tingling, tickling, pricking, or burning (paresthesia); depression (as an aftermath), thermoregulation dysfunction, and problems of movement and balance.3,4
Although MS is a progressive disease, it can present differently as there are four different types of MS known. These types include relapsing remitting, secondary progressive, primary progressive, and progressive relapsing.1 These exacerbations can occur in all four types of MS and can cause limitations in body structure and function, activity level, and participation level. This can lead to limitations worsening into long-term disability and decreased function.5 To decrease the progressive effects of the disease, physical therapists take a direct and indirect approach. Aquatic therapy is one recommended intervention for individuals with MS. The natural buoyancy and viscosity of water can potentially provide a safe and protective environment for individuals with MS to undertake exercise by making it easier to move their extremities without the fear of falling. The cooling effect of 85°F (the temperature of a typical swimming pool and more than 10°F cooler than human body temperature) also makes it possible to be active without overheating. Additionally, these activities do not require a highly competent swimming technique to reap the benefits.6,7
There is little knowledge on the relationship between aquatic exercises and the improved physical condition in individuals with MS.8 In the past 5 years, there has only been one systematic review related to MS subjects using aquatic therapy as an intervention.9 This review was limited to the effects of aquatic therapy on fatigue and quality of life (QoL). Fatigue and the wide range of symptoms that can occur with MS should be reviewed further.
The purpose of this review is to identify current research, specifically randomized controlled trials (RCTs), that examines the effectiveness of aquatic therapy for treating individuals with MS.
Methods
Search Strategy
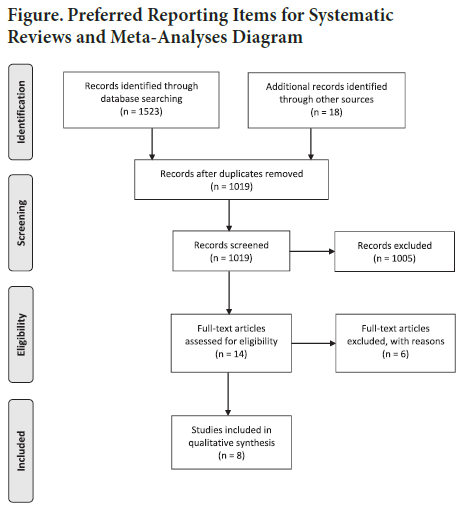
Studies were searched in March 2019 from the following databases: Academic Search Elite, Academic Search Premier, CINAHL Complete, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Cochrane Clinical Answers, MEDLINE, MEDLINE with Full Text, and SPORTDiscus with Full Text. Key words included “‘multiple sclerosis’ or ‘ms’ or ‘demyelinating disease’ or ‘relapsing remitting’, AND “‘aquatic therapy’ or ‘hydrotherapy aquatic exercise’ or ‘water exercise’ or ‘pool therapy’ or ‘water therapy’” and “‘fatigue’ or ‘exhaustion’ or ‘tiredness’ or ‘lethargy’ or ‘endurance’ or ‘benefits.’” We limited the search to scholarly journals, RCTs, English language, and dated 2010-2019. The initial search found 1,523 articles, 522 of which were duplicates. An additional 18 articles were found on the PEDro database using the key word “multiple sclerosis” under the therapy category of “hydrotherapy, balneotherapy.” After screening of the title and abstract of the 1,019 articles, 1,005 articles were excluded due to not including the core criteria of MS, aquatic therapy intervention, and benefits from aquatic therapy. After a full-text review, six articles were removed due to not being RCTs. The eight remaining articles were included in this systematic review. Please refer to the Figure.
Article Quality Assessment
The primary investigators used the PEDro scale to assess the quality of each study. The eight articles were independently reviewed by three primary investigators (NA, BB, EH), and discrepancies were resolved by a fourth reviewer (BS). All eight studies scored good or fair. PEDro scores for each article are listed in the Table. The PEDro scale is based on the Delphi list, a list for quality assessment of RCTs for conducting systematic reviews. It is a 10-point scale used for internal validity (criteria 2-9) and interpretable statistical information (criteria 10 and 11). Scores of 9 or 10 are considered excellent, 6-8 are good, 4 or 5 are fair, and <4 are poor. Criteria are based on random and concealed allocation, baseline comparability, blinding, follow-up, intention to treat, between-group comparisons, point estimates, and variability. Points are only awarded when a criterion is clearly satisfied in the study. This tool is not a measurement of the validity of a study’s conclusions and should not be used as a tool for the clinical usefulness of a study. It should also not be used to compare the quality of different therapy trials, because it is not possible for some types of therapy to fulfill all criteria.
Results
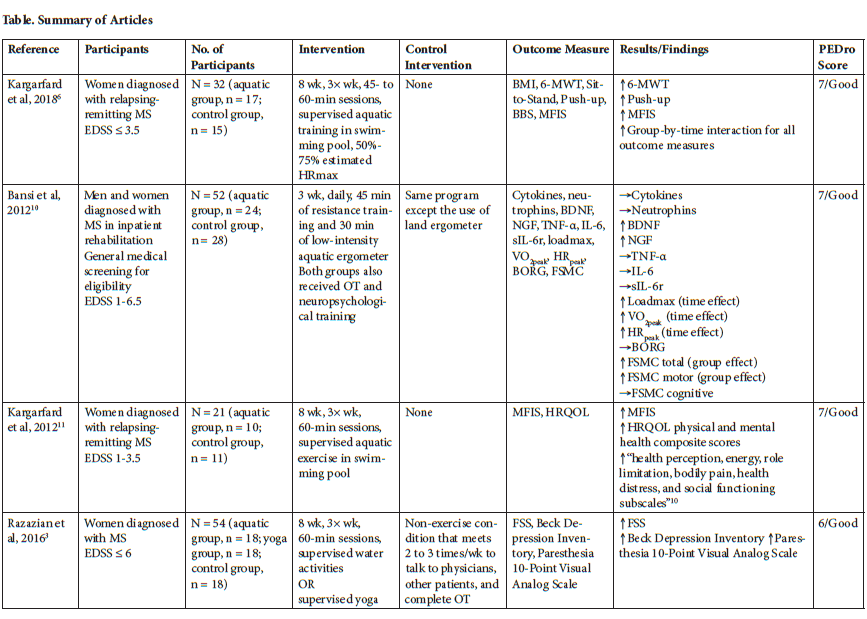
According to the PEDro score assigned to each article, five articles were categorized as good and three articles were categorized as fair. In total, 305 subjects were included in the analyses. All participants were diagnosed with MS and had an Expanded Disability Status Scale (EDSS) score from 0 to 7.5. EDSS is used to quantify disability in individuals with MS. Please refer to the summary of articles in the Table. In Kargarfard et al6, the experimental aquatic intervention group had improvements in all six outcome measures including body mass index, 6-Minute Walk Test (6-MWT), the Sit-to-Stand test, Push-up test, Berg Balance Scale (BBS), and Modified Fatigue Impact Scale (MFIS). By contrast, the control group had worsening or a deterioration of results within all of the outcome measures. For all of the outcome measures, there were significant group-by-time interactions between the experimental and control groups. Significant improvements within the experimental group were evident for the 6-MWT, Push-up test, and MFIS. Aquatic therapy was also shown to significantly improve the MFIS scores, as well as QoL, in patients with relapsing-remitting MS in Kargarfard et al.11 The Bansi et al10 compared the intervention of aquatic ergometery to the control group of land ergometry. This study showed no significant difference in the blood serum levels of cytokines and neutrophins after 3 weeks of training. It did, however, show a significant increase in brainderived neurotrophic factor and nerve growth factor. No differences were found for the tumor necrosis factor α, interleukin- 6 (IL-6), and soluble receptor of IL-6. Significant time effect differences were shown in the aquatic group for maximum workload in watts (loadmax), peak oxygen consumption (VO2peak), and peak heart rate (HRpeak) all achieved during cardiopulmonary exercise testing. On the Fatigue Scale for Motor and Cognitive Functions (FSMC), significant group effect differences were evident for the FSMC total score and the motor function subscore.
According to Razazian et al,3 aquatic exercise significantly improved fatigue, depression, and paresthesia in female patients with MS. This study utilized self-rating questionnaires including the Fatigue Severity Scale (FSS), Beck Depression Inventory, and a 10-Point Visual Analog Scale (VAS) to assess paresthesia. Significant improvements were found for fatigue, depression, and paresthesia for the all factors of time, group, and time-group interactions.
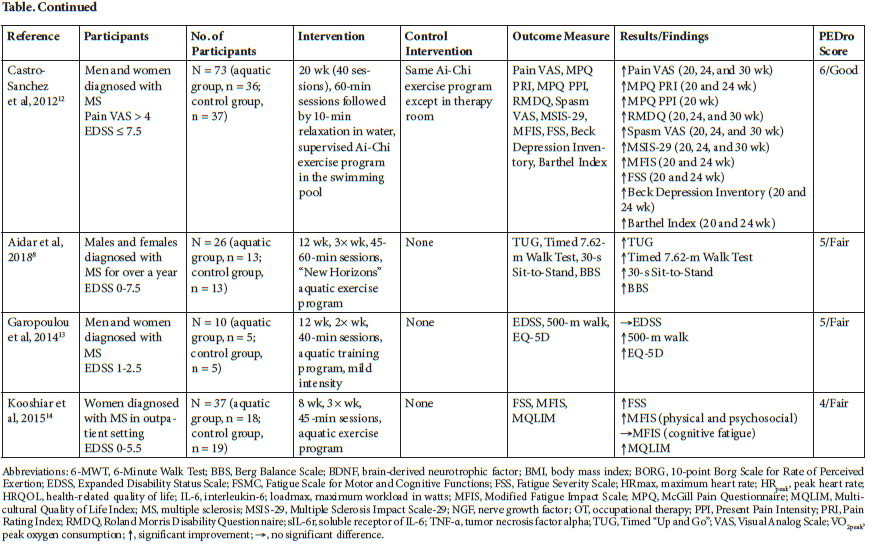
In Castro-Sanchez et al,12 a 20-week Ai-Chi aquatic exercise program showed a significant pain reduction in MS patients that lasted for 10 weeks after the program. It also improved disability, depression, and fatigue. Multiple outcome measures were taken at baseline and at 20, 24, and 30 weeks. The primary outcome measures included the Pain VAS, the Pain Rating Index, and Present Pain Intensity (PPI) from the McGill Pain Questionnaire (MPQ) and Roland Morris Disability Questionnaire (RMDQ). The study also utilized secondary outcome measures of spasm VAS, Multiple Sclerosis Impact Scale-29 (MSIS-29), MFIS, FSS, Becks Depression Inventory, and Barthel Index. Significant changes in the experimental aquatic group from baseline are indicated in the Table. No significant changes were found in the control groups for any of the measures, with the exception of the Roland Morris Disability Scale Questionnaire at weeks 20 and 24 and the MSIS-29 psychological score at 20 weeks. Multiple significant differences between the experimental and control groups were also found at varying weeks for pain, disability, spasm, MSIS-29, MFIS physical, fatigue, and depression.
Aidar et al8 found significant improvements in the experimental group for the Timed “Up and Go” (TUG) Test, Timed 7.62-Meter Walk Test, 30-s Sit-to-Stand test, and the BSS. The authors hypothesized that a 12-week aquatic therapy program would improve muscle strength and physical condition. Findings of this study support the use of aquatic therapy to improve the functional mobility of individuals with MS by “improving their lower limb muscle strength, walking, sitting and standing” as well as balance.
In Garopoulou et al,13 walking ability was assessed by two neurologists using the EDSS as the participants walked on a treadmill. No significant changes were noted in the EDSS scores for either groups. Walking ability was also measured by a 500-m walk test on the treadmill with the time required to complete the test recorded electronically. QoL was measured using the EuroCol 5 Dimensions (EQ-5D) questionnaire, which assesses “mobility, self-care, usual activities, pain/discomfort and anxiety/depression.”13 The aquatic intervention group showed significant improvements on the EQ-5D and 500-m walk test. The control group had a significant worsening of scores on both tests.
Finally, Kooshiar et al14 had significant improvements in physical and psychosocial fatigue perception, QoL, and fatigue severity, but no change was indicated in the cognitive fatigue perception. Significant effects were shown in the pre- and post-intervention factors as well as between groups. Outcome measures included the MFIS (with subgoals of physical, psychosocial, and cognitive functioning domains), FSS, and Multicultural Quality of Life Index (MQLIM).
Discussion
Currently, there is limited research on aquatic therapy as an exercise intervention for individuals with MS. Limiting the search to RCTs within the last decade further eliminated potential studies for this review. The consensus of all eight articles is that aquatic therapy has many positive effects for individuals with MS.
Fatigue
The most common benefit throughout the studies was the improvement on fatigue. “Fatigue is defined as a subjective feeling of lack of energy to start and continue an activity, which is not related to depression, or muscle weakening.”15 Six of the eight studies measured fatigue by using various outcome measures. Five of these six articles found fatigue to be significantly improved. Four of the studies that showed fatigue improvement had very similar intervention strategies. The subjects participated in aquatic therapy for 8 weeks, three times per week, and for between 45 and 60 min each session. Kooshiar et al’s “trial determined that eight weeks of aquatic therapy can decrease fatigue severity, and the physical and psychosocial domains of fatigue perception in MS patients.”14 Castro-Sanchez et al12 established a slightly longer intervention of 20-week Ai-Chi exercise program in the pool twice per week and also showed improvements with fatigue symptoms. The one study that did not show improvements related to fatigue was the Bansi et al10 trial. A possible reason for this discrepancy could be the aquatic intervention dosing. Patients in the Bansi et al10 study were recruited from a rehabilitative stay with a mean duration of 3 weeks and daily training that may have caused subjects to remain fatigued. The fatigue may have not improved because the duration was not long enough or the frequency was too often to capture fatigue improvements.
The outcome measures for fatigue used in these studies were the MFIS, FSS, or both. In the five studies that showed improvement in fatigue, the improvement was in either perception, severity, or both. The control groups in these studies did not show as much improvement in fatigue symptoms compared with aquatic therapy groups. For example, using the FSS “the experimental group showed a significant reduction in fatigue at week 20 (P < 0.043) and week 24 (P <0.046). The control group showed no significant differences versus baseline at any point throughout the study, with only 12% evidencing an improvement. Additionally, the aquatic exercise group and the control group significantly differed in scores at week 24 (P < 0.048).”12 The Kooshair et al14 clinical trial also found that “aquatic exercise significantly decreased fatigue severity and perception.” Although the Kargarfard et al11 and Razazian et al3 clinical trials were limited to females with MS, they also found positive improvement with fatigue for their subjects that performed aquatic exercises. A couple reasons for this were hypothesized, one being the improvement with thermoregulation, but the other explanation by Kargarfard et al11 is that “the buoyant effect of water can decrease gravity and resistance against body movements and assist MS patients in enduring longer periods of physical activity with less fatigue.”
Balance
Two of the eight RCTs addressed the effects that aquatic therapy had on balance of individuals with MS. The studies performed by Aidar et al8 and Kargarfard et al6 both used the BBS to collect data on this variable. The BBS is a 14-item scale that is used to assess static and dynamic balance as well as fall risk. Items are scored on a 0- to 4-item scale, with the maximum score being 56. In both studies, balance was improved in the experimental groups. In the Kargarfard et al6 study, there was a significant group-by-time interaction. In the Aidar et al8 study, the BBS scores significantly improved in the aquatic exercise group compared with baseline. Kargarfard et al6 stated, “In participants with MS, loss of balance is a significant issue because of poor judgment as well as reduced power and motion control.” The reduction of power and motor control is a large factor in fall risk for individuals with MS. Evidence supports aquatic therapy as a beneficial mean for improving balance for individuals with MS.
Depression
The studies performed by Razazian et al3 and Castro-Sanchez et al12 examined depression using the Beck Depression Inventory. The Beck Depression Inventory is a 21-item questionnaire that asks about depressive mood, loss of appetite, sleep disorders, and suicidality. It uses a 4-point scale, with 0 being no change and 3 being dramatic change. Higher scores reflect a greater severity of depressive symptoms. 3 In the Razazian et al3 study, depression was examined at baseline as well as at the end of the study, 8 weeks later. At the end of the 8-week program, the control group had no change and stayed in the moderate-to-severe depression categories. As for the experimental group, subjects were in the no/minimal or mild depression categories following the 8-week program. “Compared with a nonexercise condition, both yoga and aquatic exercising three times a week for eight consecutive weeks positively influenced fatigue, depression, and paresthesia in female patients with MS.”3 In the Castro- Sanchez et al12 study, experimental and control groups were evaluated pretreatment, immediately following treatment, 4 weeks after treatment, and 10 weeks after treatment. The experimental group showed a significant reduction at weeks 20 (p < 0.028) and 24 (p < 0.040), whereas the control group showed no significant difference versus baseline at any time.
Quality of Life
QoL has historically been defined in several ways. The generally accepted idea of QoL is that it is “a multidimensional concept that focuses on the impact of disease and its treatment on the well-being of an individual” and is “influenced by our physical and social environment as well as our emotional and existential reactions to that environment.”16 QoL is a term used in several medical settings and could indicate how well a patient responds to treatment. Therefore, the primary investigators of this review deem QoL to be an important factor to consider in the MS population. The studies in this review that measured QoL as a primary outcome include the Kooshiar et al,14 Garopoulou et al,13 and Kargarfard et al6 studies. None of the studies included its own definition of QoL, but all three studies agree that people with MS display lower levels of QoL than the general population. Each study presented slightly different aquatic exercise intervention protocols based on types of exercise, frequency, and duration. Garopoulou et al13 measured QoL with the EQ-5D questionnaire, Kooshiar et al14 measured the MQLIM, and Kargarfard et al6 measured the Multiple Sclerosis Quality of Life-54. Even with these differences in protocol and measurement, each study measured significant improvements in QoL.6,13,14 The Garopoulou et al13 study resulted in a slightly higher p-value interaction effect than the other studies, and this could be related to the less frequent protocol (2 times per week, 12 weeks). This could indicate that higher frequency dosing can lead to greater improvements in QoL in a shorter duration of time. The tools used in each study account for several factors related to QoL, which may indicate that improvements were made in multiple areas of the participants’ lives that contribute to their overall QoL.
Pain
Although the Kooshiar et al,14 Garopoulou et al,13 and the Kargarfard et al6 trials all had pain dimensions in their QoL measurements and the Razazian et al3 trial used questionnaires to measure paresthesia, only the Castro-Sanchez et al12 trial focused on pain. The trial intervention was an Ai- Chi exercise program in which the subjects performed slow, relaxing big movements in a pool at shoulder depth. Another positive note to this trial was that subjects needed to have a pain VAS rating ≥4 to be included. The control group in this trial performed the same relaxation exercises as the aquatic group, but did not get the Ai-Chi interventions in the pool. Throughout the trial, the subjects who performed aquatic exercises showed significant improvements on the Pain VAS, MPQ PRI, and MPQ PPI, whereas the control group did not. “The experimental group showed a significant reduction (P < 0.034) in PPI at week 20. The control group showed no significant difference with baseline PPI scores at any time point, and no significant difference between the groups was observed at any time point.”12
Walking Ability
Walking is functional and an important measurement to consider in individuals with walking disability. Garopoulou et al13 concluded that “walking deficits constitute a decisive factor for the overall decline of walking patients with MS since it negatively affects the activities associated with daily schedule and QoL of patients with MS.” This study showed a significant improvement in walking mobility (time to walk 500 m on a treadmill) in the intervention group compared with the control group by 584.2% (p < 0.05) and that walking mobility significantly improved in the intervention group by 7.6% (p < 0.05). However, no significant changes were seen in the EDSS measurement of walking ability within or between groups as both groups stayed at a very low mean rating of disability. 13 Therefore, aquatic exercise resulted in a higher average walking speed over 500 m. The Aidar et al8 study utilized different measurements of walking ability than the Garopoulou et al13 study. Instead of measuring time over a long distance, Aidar et al8 measured walking ability with the TUG test and the Timed 7.62-Meter Walk. Significant improvements were noted in both outcome measures. The TUG measurement of walking ability incorporates body “strength, agility and balance”, whereas the Timed 7.62-Meter Walk is a measurement of “lower limb function present in the multiple sclerosis functional composite (MSFC).”8 Both activities represent more of a household ambulation function of short spurts of activity rather than community ambulation function like the 500-m walk test. These findings in both studies signify aquatic therapy as an effective intervention for improving household and community ambulation in people with MS.
Conclusions
This systematic review supports a wide array of effects for individuals with MS participating in aquatic therapy. Overall, the evidence supports that aquatic therapy is beneficial for individuals with MS improving fatigue, pain, depression, balance, walking ability, and QoL. Limitations to this systematic review included the variation of intervention protocols, EDSS scores, and outcome measures, making it difficult to compare any two articles’ results. Future research could investigate the positive cooling effects that submersion has on the body’s core temperature. Heat sensitivity is a well-known symptom of MS, but there is very little research on this topic. Most of the studies reviewed included lightto- moderate intensity exercise. Therefore, future research could also investigate the effects of higher intensities with aquatic therapy.
References
1. Widener GL. Multiple sclerosis. In: Umphred DA, Lazaro RT, Roller ML, Burton GU, eds. Umphred’s Neurological Rehabilitation. 6th ed. St Louis, MO: The CV Mosby Co; 2013;585-600.
2. Goldenberg M. Multiple sclerosis review. Pharm Ther. 2012;37(3):175-183.
3. Razazian N, Yavari Z, Farnia V, et al. Exercising impacts on fatigue, depression, and paresthesia in female patients with multiple sclerosis. Med Sci Sports Exerc. 2016;48(5):796-803. doi:10.1249/ MSS.0000000000000834.
4. Davis SL, Wilson TE, White AT, Frohman EM. Thermoregulation in multiple sclerosis. J Appl Physiol. 2010;109(5):1531-1537.
5. Concert G, Haller L, Kaminsky E, et al. Communitybased aquatic programme for individuals with multiple sclerosis: a pilot study. Disabil Rehabil. 2011;33(9):720- 728. doi:10.3109/09638288.2010.507855.
6. Kargarfard M, Shariat A, Ingle L, Cleland JA, Kargarfard M. Randomized controlled trial to examine the impact of aquatic exercise training on functional capacity, balance, and perceptions of fatigue in female patients with multiple sclerosis. Arch Phys Med Rehabil. 2018;99(2):234-241. doi:10.1016/j. apmr.2017.06.015.
7. Butler C. Walking in water. Inside MS. 2002;20(3):66.
8. Aidar FJ, Gama de Matos D, de Souza RF, et al. Influence of aquatic exercises in physical condition in patients with multiple sclerosis. J Sports Med Phys Fitness. 2018;58(5):684-689. doi:10.23736/ S0022-4707.17.07151-1.
9. Willis KR, Barnes LJ, Hewes G, Phonogam NR. The effects of aquatic therapy on fatigue and quality of life in patients with multiple sclerosis: a systematic review. Aquatic Physical Therapy Section Platforms Presented at APTA’s 2017 Combined Sections Meeting in San Antonio, Texas. J Aquat Phys Ther. 2017;25(2):69.
10. Bansi J, Bloch W, Gamper U, Kesselring J. Training in MS: influence of two different endurance training protocols (aquatic versus overland) on cytokine and neurotrophin concentrations during three week randomized controlled trial. Mult Scler. 2012;19(5):613-621. doi:10.1177/1352458512458605.
11. Kargarfard M, Etemadifar M, Baker P, Mehrabi M, Hayatbakhsh R. Effect of aquatic exercise training on fatigue and health-related quality of life in patients with multiple sclerosis. Arch Phys Med Rehabil. 2012;93(10):1701- 1708. doi:10.1016/j.apmr.2012.05.006.
12. Castro-Sánchez AM, Matarán-Peñarrocha GA, Lara- Palomo I, Saavedra-Hernández M, Arroyo-Morales M, Moreno-Lorenzo C. Hydrotherapy for the treatment of pain in people with multiple sclerosis: a randomized controlled trial. Evid Based Complement Alternat Med. 2012;2012:473963. doi:10.1155/2012/473963.
13. Garopoulou V, Tsimaras V, Orologas A, Mavromatis I, Taskos N, Christoulas K. The effect of an aquatic training program on walking ability and quality of life of patients with multiple sclerosis. J Physic Edu Sport. 2014;14(1):106. doi:10.7752/jpes.2014.01017.
14. Kooshiar H, Moshtagh M, Sardar MA, Foroughipour M, Shakeri MT, Vahdatinia B. Fatigue and quality of life of women with multiple sclerosis: a randomized controlled clinical trial. J Sports Med Phys Fitness. 2015;55(6):668-674.
15. Pasiut S, Juda K, Mirek E, Szymura J. The effect of rehabilitation on the perceived level of fatigue of patients with multiple sclerosis. Physiotherapy/Fizjoterapia. 2015;23(1):3-10.
16. Fairclough DL. Design and Analysis of Quality of Life Studies in Clinical Trials. Boca Raton, FL: CRC Press/ Chapman & Hall Book; 2010;2-3.
