The Influence of Cognition Impairment on the Fitness-Cognition Relationship in Multiple Sclerosis

Selected By
Lori Mayer, DNP, MSN, RN, MSCN
Why is this study important to me?
The present study provides evidence that there is a significant association between cardiorespiratory fitness and processing speed in persons with MS-related PSI. Such an investigation provides support for aerobic exercise training as a possible behavioral approach for managing/treating MS-related cognitive impairment, beyond merely improving cognitive performance.
What was the objective of this article?
Cognitive dysfunction is a major concern among persons with MS, as around half demonstrate impairment, particularly processing speed impairment (PSI). PSI is associated with depression, unemployment, decreased performance of daily activities, and a lower quality of life for those living with MS. Currently, there are no FDA-approved treatments for MS-related PSI, and there is mixed evidence supporting exercise training as a behavioral therapy for improving PSI.
This article seeks to identify if exercise training is associated with PSI, and if exercise can potentially improve cognitive processing speed in people living with MS.
How did the authors study this issue?
The study looked at 64 persons with relapsing–remitting MS, both with and without MS-related PSI, and examined the associations between cardiorespiratory fitness and processing speed. This investigation sought to provide the first evidence for the potential development of an aerobic exercise training intervention for directly addressing MS-related PSI, beyond merely improving cognitive performance.
| SHARE: | |||||
Original Article
The Influence of Cognitive Impairment on the Fitness–Cognition Relationship in Multiple Sclerosis
Brian M. Sandroff, Robert W. Motl, and John Deluca
Medicine & Science in Sports & Exercise
Abstract
Introduction: Cognitive processing speed impairment (PSI) is common and debilitating in persons with multiple sclerosis (MS). Exercise training has been proposed as a behavioral approach for possibly managing MS-related processing speed dysfunction, largely based on cross-sectional studies of the relationship of cardiorespiratory fitness and cognitive processing speed. However, there is minimal evidence supporting exercise training as a treatment for MS-related PSI, as the vast majority of the existing studies have examined exercise and cardiorespiratory fitness effects on cognition in samples of noncognitively impaired persons with MS. To that end, the current cross-sectional investigation examined whether cardiorespiratory fitness was differentially associated with processing speed in persons with MS with and without PSI.
Methods: Sixty-four persons with MS undertook the Symbol Digit Modalities Test for establishing groups with and without MS-related PSI, a modified flanker task for measuring processing speed performance, and an incremental exercise test to exhaustion on a cycle ergometer for measuring cardiorespiratory fitness in a single testing session. Bivariate correlations were performed on cardiorespiratory fitness and processing speed outcomes in PSI group subsamples.
Results: In the sample without PSI, cardiorespiratory fitness was not significantly associated with processing speed (P = 0.08). However, in the sample with PSI, cardiorespiratory fitness was significantly associated with processing speed (P = 0.01), such that lower cardiorespiratory fitness was strongly associated with slower processing speed.
Conclusions: This study provides preliminary evidence of a significant association between cardiorespiratory fitness and processing speed in persons with MS-related PSI. Such an investigation provides the first direct support for aerobic exercise training as a possible behavioral approach for managing/treating MS-related cognitive impairment, beyond merely improving cognitive performance.
Multiple sclerosis (MS) is a common, neurological disease that is initially characterized by inflammatory processes and demyelination in the CNS (14). The disease eventually becomes neurodegenerative, leading to irreversible damage to gray and white matter in the brain (9,34); such CNS damage manifests in the accumulation of physical and cognitive disability. Cognitive dysfunction is a major concern among persons with MS, as upward of half of patients demonstrate impairment on objective neuropsychological tests, particularly on those addressing cognitive processing speed (6). Of note, there is evidence suggesting that generalized MS-related cognitive impairment might be a by-product of a fundamental deficit in processing speed (i.e., relative consequence model [10]). Processing speed impairment (PSI) has a substantial effect on the lives of those with MS, considering its association with depression (2), unemployment (17), reduced ability to perform activities of daily living (12), and poor quality of life (4). There further are no FDA-approved pharmacological treatments for MS-related PSI, and there have been no published cognitive rehabilitation randomized controlled trials (RCT) for improving processing speed in those with objective PSI (1). One promising behavioral approach for potentially improving cognitive processing speed in persons with MS involves exercise training.
Overall, there is mixed evidence supporting exercise training for managing impaired processing speed in persons with MS, mostly based on a lack of well-designed class I and class II RCT as summarized in a recent systematic review (29). However, there is promising evidence supporting exercise training for improving processing speed based on a recent pilot RCT (24) and several cross-sectional studies reporting associations between better cardiorespiratory fitness (as a presumed surrogate for aerobic exercise training) and faster processing speed in persons with MS (21,22,27,28,30).
However, one issue that has been raised regarding this line of research is that a vast majority of the existing studies have examined exercise and cardiorespiratory fitness effects on cognition in samples of persons with MS who are noncognitively impaired. This is particularly problematic as persons with objective MS-related cognitive impairment represent the cohort of persons with MS who most need such interventions; there is minimal evidence that exercise training could be applied as a treatment for MS-related PSI (i.e., the most common MS-related cognitive deficit). The current cross-sectional investigation examined whether cardiorespiratory fitness was differentially associated with speed of processing in persons with MS with and without PSI. Such an investigation would provide the first evidence for informing the development of potential aerobic exercise training interventions for directly addressing MSrelated PSI, beyond merely improving cognitive performance. We established groups of persons with and without MS-related PSI based on z-scores on the Symbol Digit Modalities Test (SDMT), considering that this outcome has been highlighted as the most sensitive neuropsychological measure of MS-related PSI and has been proposed as a proxy for generalized MS-related cognitive impairment based on the relative consequence model (6,10). We further operationalized reaction time (RT) on correct trials of a modified flanker task as a measure of processing speed performance, as has been performed in exercise training interventions on cognition and cross-sectional studies informing such interventions older adults (8,13).
METHODS
Participants. The current cross-sectional examination represents a secondary analysis of data from baseline sessions of several separate investigations of the acute effects of exercise on cognitive performance in persons with MS (25,26). The overall sample included 64 persons with relapsing– remitting MS. Each study involved the same inclusion criteria: (a) definite diagnosis of MS based on physician"s confirmation of MS and its clinical course based on accepted criteria (16), (b) relapse free for the past 30 d (i.e., relative neurologic stability and not currently taking steroids), (c) self-reported ability to read 14-point font, (d) walk with or without minimal assistance (i.e., cane or crutch, but not a walker/bilateral support), (d) age between 18 and 54 yr, (e) willingness and ability to complete the cardiorespiratory fitness and speed of processing assessments, and (f ) low risk for contraindications of maximal exercise testing based on a ‘‘no’’ response to all items of the Physical Activity Readiness Questionnaire (PAR-Q [33]), or a single ‘‘yes’’ response along with a physician"s approval. We note that having a relapsing–remitting clinical disease course was not an a priori inclusion criterion. As the present study was a secondary analysis of data, we did not recruit groups a priori based on having cognitive impairment.
Cardiorespiratory fitness. Cardiorespiratory fitness was measured as peak oxygen consumption (V˙ O2peak; cardiorespiratory capacity) using an incremental exercise test performed to exhaustion on an electronically braked, computer-driven cycle ergometer (Lode BV, Groningen, The Netherlands) and a calibrated open-circuit spirometry system (TrueOne, Parvo Medics, Sandy, UT) for analyzing respiratory gases. The incremental exercise test initially involved a 3-min warm-up at 0 W. The initial work rate for the incremental exercise test was 0 W, and the work rate continuously increased at a rate of 15 WIminj1 until participants reported volitional fatigue. This protocol is valid for evaluating aerobic fitness (i.e., V˙ O2peak) in persons with MS who have Expanded Disability Status Scale (EDSS) scores ranging from 0 to 6 (18). Oxygen consumption (V˙ O2), RER, and work rate were measured continuously by the open-circuit spirometry system and expressed as 20-s averages. HR was displayed using a Polar HR monitor (Polar Electro Oy, Kempele, Finland), and HR and RPE (5) were recorded every minute. V˙ O2peak was expressed in milliliters per kilogram per minute based on highest recorded 20-s V˙ O2 value when two of four criteria were satisfied: 1) V˙ O2 plateau with increasing work rate, 2) RER Q1.10, 3) peak HR within 10 bpm of agepredicted maximum (i.e., ~1 SD), or 4) peak RPE Q17.
Cognitive processing speed. Cognitive processing speed was measured using the SDMT (31) and a modified flanker task (11). The SDMT is considered the best-characterized neuropsychological measure of processing speed in MS based on its psychometric properties (6). Further, the SDMT is often considered a proxy of generalized cognitive impairment in this population based on data that suggest that MS-related deficiencies in multiple cognitive domains (e.g., learning and memory, executive function) might be a manifestation of a primary deficit in processing speed (6,10). Briefly, this test involves rapidly pairing single-digit numbers with abstract geometric symbols, with the primary outcome being the total number of correct responses that are verbally provided in a 90-s period (i.e., raw score). We further calculated z-scores on the SDMT for characterizing impairment in cognitive processing speed using regression-based norms, controlling for age, sex, and education (20). Consistent with previous neuropsychological studies in persons with MS, we defined PSI as SDMT scores at least 1.5 SD units below the regressionbased normative score for healthy controls. The modified flanker task is a computerized neurocognitive measure of processing speed and inhibitory control (i.e., executive function). This test requires participants to inhibit task-irrelevant visual information to correctly respond to a central target stimulus as rapidly as possible. We operationalized mean RT (ms) for correct trials as a measure of complex cognitive processing speed, as has been performed in studies involving cognitive performance in older adults (13).
Disability status. All participants underwent a neurological examination by a Neurostatus-certified researcher for generation of EDSS (15) scores for describing the disability status of the sample.
Procedure. All study procedures were approved by an Institutional Review Board, and all participants provided written informed consent. The study protocol involved a single testing session whereby participants initially provided demographic and clinical information, followed by administration of the SDMT and modified flanker task in a quiet, sound-dampened room. This was followed by the brief neurological examination for generation of an EDSS score. All participants then underwent the incremental exercise test for measurement of cardiorespiratory fitness.
Data analysis. All data were analyzed using SPSS version 21 (SPSS Inc., Chicago, IL). The first analysis involved performing bivariate, nonparametric Spearman correlations (Q) between cardiorespiratory fitness and mean RT on the modified flanker task in the overall sample (23). This was followed by computing z-scores for the SDMT based on published norms (20) and identifying groups of persons with MS with PSI (i.e., SDMT scores at least 1.5 SD below the normative value) and persons without PSI. Differences between the cognitive groups in demographic and clinical characteristics (age, sex, EDSS scores, disease duration, and education), cardiorespiratory fitness, and mean RT on the modified flanker task were examined using chi-square difference tests and independent-samples t-tests. Lastly, additional bivariate Spearman correlations were performed between cardiorespiratory fitness and mean RT on the modified flanker task in the PSI group subsamples. This afforded the opportunity to compare the association between cardiorespiratory fitness and cognitive processing speed in persons with and without impaired cognitive processing speed (i.e., moderation). The associations between cardiorespiratory fitness and SDMT scores in those subsamples were not examined to avoid issues associated with multicollinearity. Values for the magnitude of correlation coefficients of 0.1, 0.3, and 0.5 were interpreted as small, moderate, and large, respectively (7). To examine whether the correlation coefficients were significantly different in magnitude between the PSI groups, Fisher"s z-test was applied.
RESULTS
Participant characteristics. Demographic and clinical characteristics of the overall sample and PSI subsamples are presented in Table 1. There were no statistically significant differences in disease duration (t62 = j0.02, P = 0.99), years of education (t62 = 1.04, P = 0.30), sex (W2 1 = 1.20, P = 0.27), or EDSS score (W2 8 = 10.29, P = 0.25) between PSI subgroups. However, there were significant subgroup differences in age (t62 = j3.16, P G 0.01), such that persons with PSI were significantly younger than those without PSI.
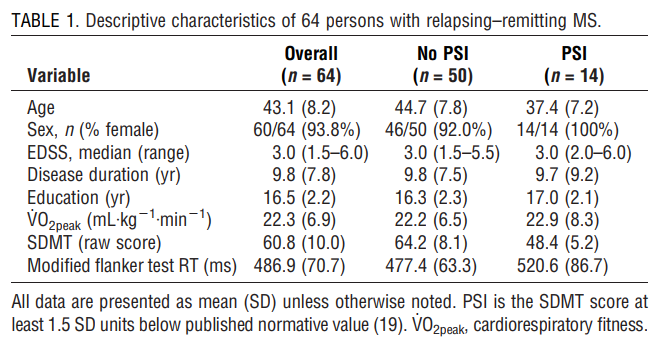
Fitness and cognitive outcomes in the overall sample and by PSI subgroup are presented in Table 1. Briefly, the overall sample demonstrated cardiorespiratory fitness levels that were consistent with those from other samples of persons with MS (28). Interestingly, there was not a PSI subgroup difference on V˙ O2peak (t62 = 0.37, P = 0.71).
Overall, the mean SDMT score was 60.8 (SD = 10.0); that value is 0.43 SD units below the regression-based normative value (that controlled for age, sex, and education) for healthy controls (20). As expected, there was a statistically significant PSI subgroup difference on SDMT raw scores (t62 = j6.88, P G 0.01) (see Table 1). Mean generalized RT on the modified flanker task for the overall sample was 486.9 ms; that value is 0.76 SD units below the mean generalized RT value for a sample of 28 healthy controls (27). There was a statistically significant PSI subgroup difference on generalized RT on the modified flanker task (t62 = 2.07, P = 0.04), such that persons with MS with PSI demonstrated longer RT on correct trials of the modified flanker task than those without PSI (see Table 1).
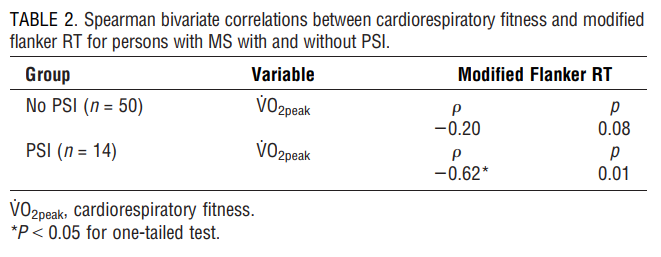
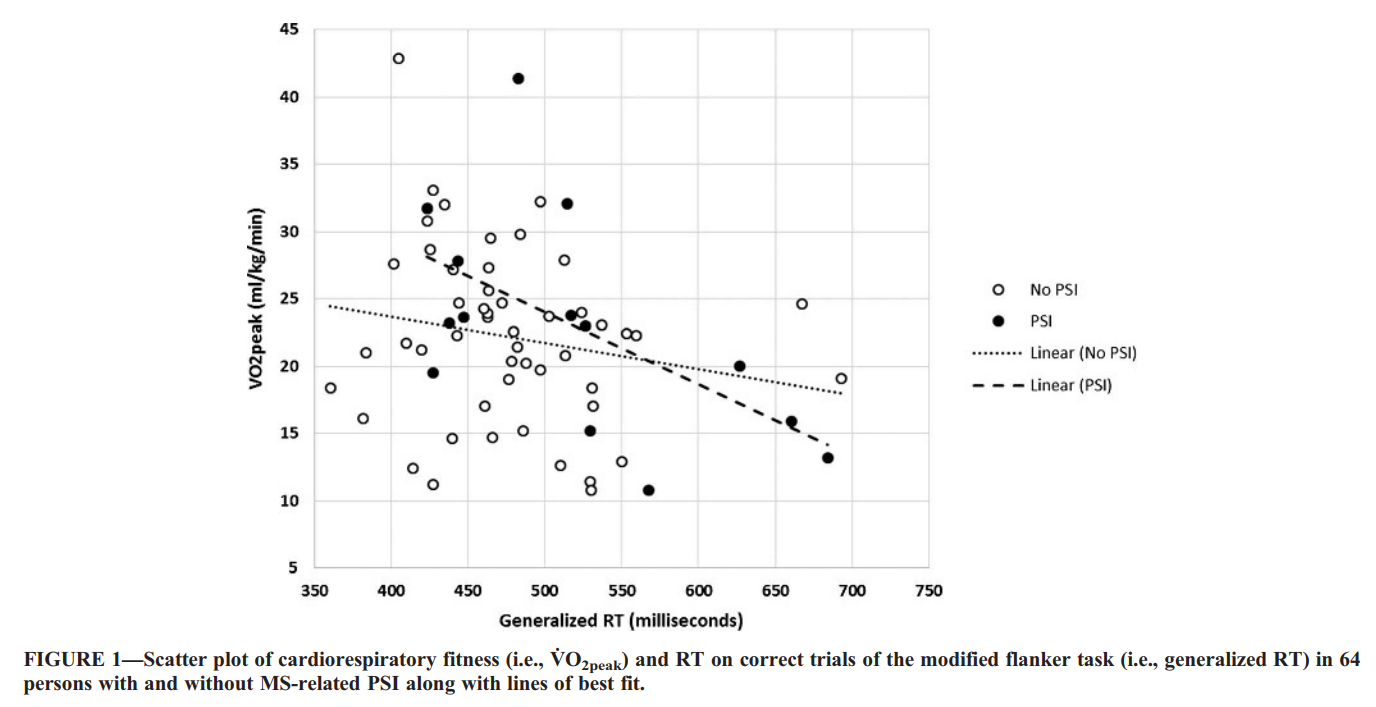
Correlations. We next conducted bivariate correlations between cardiorespiratory fitness (i.e., V˙ O2peak) and generalized RT on the modified flanker task in the overall sample and within the PSI subgroups (Table 2). The scatter plots for that association are presented in Figure 1. In the overall sample, V˙ O2peak was significantly associated with generalized RT on the modified flanker task (Q = j0.28, P = 0.01), such that lower cardiorespiratory fitness was associated with longer RT on correct trials of the modified flanker task; this association was small-to-moderate in magnitude. By comparison, in the sample without PSI, V˙ O2peak was not significantly associated with generalized RT on the modified flanker task (Q = j0.20, P = 0.08). However, in the sample with PSI, V˙ O2peak was significantly associated with generalized RT on the modified flanker task (Q = j0.62, P = 0.01), such that lower cardiorespiratory fitness was associated with longer RT on correct trials of the modified flanker task; this association was strong in magnitude. The magnitude of the correlations between cardiorespiratory fitness and processing speed was not statistically significant between PSI subgroups based on Fisher"s z-test (z = j1.56, P = 0.06).
DISCUSSION
The present study is the first to examine if cardiorespiratory fitness was differentially associated with processing speed in persons with and without MS-related PSI for better informing the development of aerobic exercise training interventions for managing MS-related cognitive impairment. Higher levels of cardiorespiratory fitness (i.e., greater V˙ O2peak values) were significantly associated with faster processing speed (i.e., shorter RT on correct trials on the modified flanker task) in the overall sample. Objective MS-related PSI was seemingly a moderator of this association, such that cardiorespiratory fitness was strongly and significantly associated with processing speed only in those with SDMT scores at least 1.5 SD below the normative score for healthy controls (i.e., 5th percentile). This suggests that improving cardiorespiratory fitness via aerobic exercise training might be able to improve processing speed over time, particularly in cognitively impaired persons with MS (i.e., those who presumably have the greatest need for such an intervention). If correct, the present study provides initial evidence for developing aerobic exercise training interventions for specifically treating MS-related PSI (i.e., the most commonly impaired cognitive domain in this population), beyond merely improving cognitive performance.
The most novel aspect of the present study is that we examined the role of cognitive impairment as a potential moderator of the fitness/cognition relationship in persons with MS. We have previously reported on statistically significant and moderate-sized correlations between cardiorespiratory fitness and aspects of cognitive processing speed in persons with mild-to-moderate MS ambulatory disability (22,24,27,28,30). However, one major limitation of those research studies was that those associations were in noncognitively impaired samples (29), thus providing minimal evidence supporting exercise training for possibly managing cognitive dysfunction in this population. The current results extend this relationship into a subsample of persons with mild-to-moderate MS ambulatory disability who present with PSI, based on SDMT scores. This highlights the potential for aerobic exercise training (i.e., improving cardiorespiratory fitness) as a behavioral approach for selectively managing MS-related PSI.
The current results add to the body of literature reporting a significant fitness/cognition relationship among persons with MS (e.g., 30). In that study, cardiorespiratory fitness was associated with cognitive processing speed in persons with mild but not moderate or severe MS ambulatory disability. Similarly, in the present study, cardiorespiratory fitness was associated with processing speed in persons with mild MS ambulatory disability; however, this association was stronger among those with substantial cognitive disability. Further, in the present study, we did not observe differences in cardiorespiratory fitness between the PSI subgroups. That is, cardiorespiratory fitness levels were relatively similar between those with and without PSI. Perhaps in those persons with mild MS ambulatory disability who present with PSI, there is a greater capacity for cardiorespiratory fitness (as a presumed surrogate for aerobic exercise training) to influence cognitive functioning. This is consistent with the results from a meta-analysis in older adults that reported stronger effects of exercise training on memory in older adults with MCI compared with noncognitively impaired older adults (32). Such a result further may reflect the concept of cognitive–motor coupling in persons with MS whereby co-occurring neural damage may underlie both physical/motor and cognitive functions (3,19). Interestingly, in the present study, EDSS scores (i.e., a proxy of MS-related ambulatory disability) were more strongly correlated with SDMT raw scores (i.e., a proxy of MS-related cognitive disability) in persons with PSI compared with those without PSI (z = j3.13, P G 0.01). Future research might consider including neuroimaging measures to examine the influence of neural damage (i.e., T2 lesion volume; gray/white matter atrophy) on the fitness/cognition relationship in persons with MS who present with PSI.
There are several important limitations associated with the present study. First, the subsamples of persons with mild MS ambulatory disability with and without PSI were not recruited a priori based on SDMT scores. This would have afforded the opportunity to better match the groups on age, and perhaps better increase the generalizability of the results among fully ambulatory persons with MS who present with cognitive impairment. This further would have allowed for the recruitment of relatively equal size subsamples, considering the small sample of persons with PSI. Another limitation is that we did not administer other neuropsychological tests of processing speed (i.e., Paced Auditory Serial Addition Test) that have published regression-based normative scores for persons with MS (20) for better characterizing PSI. Rather, the present study was a secondary analysis of data from baseline sessions of three acute exercise studies in separate samples of persons with relapsing– remitting MS that did not involve the baseline administration of those tests (25,26). To that end, we were unable to examine the relationships among cardiorespiratory fitness, processing speed, and cognitive impairment in those with progressive MS or those with severe MS ambulatory disability. However, based on previously published work, we would not have expected significant associations between measures of cardiorespiratory fitness and processing speed in those MS cohorts (30). Finally, the study involved a cross-sectional experimental design such that the primary results do not indicate causality between measures of cardiorespiratory fitness and processing speed in persons with MS-related PSI. However, performing initial crosssectional analyses is important for informing the development of longitudinal RCT of aerobic exercise training (i.e., improving cardiorespiratory fitness) for potentially managing MS-related PSI before investing considerable time and resources into such a trial.
CONCLUSIONS
The present study provides preliminary evidence of a significant association between cardiorespiratory fitness and processing speed in persons with MS-related PSI. Such an investigation provides the first direct support for aerobic exercise training as a possible behavioral approach for managing/treating MS-related cognitive impairment, beyond merely improving cognitive performance. Future research efforts might focus on the continued systematic development of aerobic exercise training interventions for managing PSI in persons with MS.
The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The results of the present study do not constitute endorsement by the American College of Sports Medicine. The authors report no conflicts of interest. This study was supported in part by a grant from the Consortium of Multiple Sclerosis Centers and grant nos. MB 0024 and CA 1069-A-7 from the National Multiple Sclerosis Society.
REFERENCES
1. Amato MP, Langdon D, Montalban X, et al. Treatment of cognitive impairment in multiple sclerosis: position paper. J Neurol. 2013;260: 1452–68.
2. Arnett PA, Barwick FH, Beeney JE. Depression in multiple sclerosis: review and theoretical proposal. J Int Neuropsychol Soc. 2008;14(5): 691–724.
3. Benedict RHB, Holtzer R, Motl RW, et al. Upper and lower extremity motor function and cognitive impairment in multiple sclerosis. J Int Neuropsychol Soc. 2011;17(4):643–53.
4. Benedict RHB, Wahlig E, Bakshi R, et al. Predicting quality of life in multiple sclerosis: accounting for physical disability, fatigue, cognition, mood disorder, personality, and behavior change. J Neurol Sci. 2005;231(1–2):29–34.
5. Borg G. Borg"s Perceived Exertion and Pain Scales. Champaign (IL): Human Kinetics; 1998. p. 104.
6. Chiaravalloti ND, DeLuca J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008;7:1139–51.
7. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988. p. 567.
8. Colcombe S, Kramer AF, Erickson KI, et al. Cardiovascular fitness, cortical plasticity, and aging. Proc Natl Acad Sci U S A. 2004;101(9): 3316–21.
9. Confavreux C, Vukusic S. Natural history of multiple sclerosis: a unifying concept. Brain. 2006;129:606–16.
10. DeLuca J, Chelune G, Diamond BJ, Christodoulou C, Chiaravalloti ND. Is speed of processing or working memory the primary information processing deficit in multiple sclerosis? J Clin Exp Neuropsychol. 2004;26(4):550–62.
11. Eriksen BA, Eriksen C. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept Psychophys. 1974;16(1):143–9.
12. Goverover Y, Strober L, Chiaravalloti N, DeLuca J. Factors that moderate activity limitation and participation restriction in people with multiple sclerosis. Am J Occup Ther. 2015;69(2):1–9.
13. Holtzer R, Mahoney J, Verghese J. Intraindividual variability in executive functions but not speed of processing or conflict resolution predicts performance differences in gait speed in older adults. J Gerontol A Biol Sci Med Sci. 2014;69(8):980–6.
14. Kingwell E, Marriott JJ, Jette´ N, et al. Incidence and prevalence of multiple sclerosis in Europe: a systematic review. BMC Neurol. 2013;13:128–40.
15. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33:1444–52.
16. Lublin FD. New multiple sclerosis phenotypic classification. Eur Neurol. 2014;72(1 Suppl):1–5.
17. Morrow SA, Drake A, Zivadinov R, Munschauer F, WeinstockGuttman B, Benedict RHB. Predicting loss of employment over three years in multiple sclerosis: clinically meaningful cognitive decline. Clin Neuropsychol. 2010;24:1131–45.
18. Motl RW, Fernhall B. Accurate prediction of cardiorespiratory fitness using cycle ergometry in minimally disabled persons with relapsing–remitting multiple sclerosis. Arch Phys Med Rehabil. 2012;93(3):490–5.
19. Motl RW, Sandroff BM, DeLuca J. Exercise training and cognitive rehabilitation: a symbiotic approach for rehabilitating walking and cognitive functions in multiple sclerosis? Neurorehabil Neural Repair. 2016;30(6):499–511.
20. Parmenter BA, Testa SM, Schretlen DJ, Weinstock-Guttman B, Benedict RH. The utility of regression-based norms in interpreting the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J Int Neuropsychol Soc. 2010;16:6–16.
21. Prakash RS, Snook EM, Erickson KI, et al. Cardiorespiratory fitness: a predictor of cortical plasticity in multiple sclerosis. Neuroimage. 2007;34:1238–44.
22. Prakash RS, Snook EM, Motl RW, Kramer AF. Aerobic fitness is associated with gray matter volume and white matter integrity in multiple sclerosis. Brain Res. 2010;1341:41–51.
23. Rousselet GA, Pernet CR. Improving standards in brain-behavior correlation analyses. Front Hum Neurosci. 2012;6:119.
24. Sandroff BM, Balto JM, Klaren RE, Sommer SK, DeLuca J, Motl RW. Systematically developed pilot randomized controlled trial of exercise and cognition in persons with multiple sclerosis. Neurocase. 2016;22(5):443–50.
25. Sandroff BM, Hillman CH, Benedict RHB, Motl RW. Acute effects of walking, cycling, and yoga exercise on cognition in persons with relapsing–remitting multiple sclerosis without impaired cognitive processing speed. J Clin Exp Neuropsychol. 2015;37(2):209–19.
26. Sandroff BM, Hillman CH, Benedict RH, Motl RW. Acute effects of varying intensities of treadmill walking exercise on inhibitory control in persons with multiple sclerosis: a pilot investigation. Physiol Behav. 2016;154:20–7.
27. Sandroff BM, Hillman CH, Motl RW. Aerobic fitness is associated with inhibitory control in persons with multiple sclerosis. Arch Clin Neuropsychol. 2015;30(4):329–40.
28. Sandroff BM, Motl RW. Fitness and cognitive processing speed in persons with multiple sclerosis: a cross-sectional investigation. J Clin Exp Neuropsychol. 2012;34(10):1041–52.
29. Sandroff BM, Motl RW, Scudder MR, DeLuca J. Systematic, evidence-based review of exercise, physical activity, and physical fitness effects on cognition in persons with multiple sclerosis. Neuropsychol Rev. 2016;26(3):271–94.
30. Sandroff BM, Pilutti LA, Benedict RHB, Motl RW. Association between physical fitness and cognitive function in multiple sclerosis: does disability status matter? Neurorehabil Neural Repair. 2015;29(3):214–23.
31. Smith A. Symbol Digit Modalities Test: Manual. Los Angeles (CA): Western Psychological Services; 1982. p. 1.
32. Smith PJ, Blumenthal JA, Hoffman BM, et al. Aerobic exercise and neurocognitive performance: a meta-analytic review of randomized controlled trials. Psychosom Med. 2010;72:239–52. 33. Thomas S, Reading J, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci. 1992;17: 338–45. 34. Trapp BD, Nave KA. Multiple sclerosis: an immune or neurodegenerative disorder? Annu Rev Neurosci. 2008;31:247–69.


