Secondary Health Conditions in Individuals With Multiple Sclerosis

Selected By
Colleen Harris, MN, NP, MSCN, MSCS
Why is this important to me?
If you have MS, you may also experience other health conditions such as migraine headaches, heart disease, depression, or others. These conditions are called secondary health conditions or co-morbidities. The frequency with which secondary health conditions tend to occur in people with MS compared to the general population, including how rates of health conditions change with age, are not clear. Some studies have suggested that people with MS develop other health conditions at a younger age than the general population, called “faster aging”.
What is the objective of this study?
The authors compared the rates of secondary health conditions in people with MS and to individuals of the same age in the general population. Participants with MS were asked if they also had:
- Depression
- Migraine headaches
- Some forms of arthritis
- Cancer
- Coronary artery disease
- Diabetes
The frequency of co-morbidities among individuals with MS compared to the general population are as follows:
- Depression was 55%, and that in the general population was only 3%.
- Migraine headaches was 37%, and that in the general population was 17%.
- Arthritis was 32%, and that in the general population was 25%.
- Cancer was 15%, and that in the general population was 9%.
- However, the frequency of coronary artery disease or diabetes was not different between people with MS and the general population.
As one might expect, frequency of cancer and arthritis tend to increase with age among both individuals with MS and the general population. Migraine headaches tend to be more common among younger people with MS.
If you have MS, you may tend to have more secondary health conditions than the general population, and these conditions may occur at a different age. Regarding depression, the longer individuals live with a chronic disease such as MS, the better they appear to be at learning strategies to adapt to the disease, thereby, decreasing the tendency for depression with age. Migraine headaches may be related to the location of MS lesions, and these headaches are more common in younger people with MS than older people with MS. This study captured information at only one time point, and studies that collect information from the same person at different time points are needed to observe the natural course of secondary health conditions.
How did the authors study this issue?
The authors surveyed 339 people with MS who were members of the Gateway Chapter of the National MS Society (parts of Missouri and Illinois). Participants were asked “Have you EVER been told by a doctor or other health professional that you had…” followed by six conditions: coronary artery disease, migraine headaches, diabetes, cancer, some forms of arthritis, or depression. The participants were compared across all ages as well as within specific age categories. Most people with MS who participated were Caucasian (92%) and female (77%). The average age of MS symptom onset was 48.3 years.
| SHARE: | |||||
Original Article
Secondary Health Conditions in Individuals With Multiple Sclerosis: A Cross-Sectional Web-Based Survey Analysis
Journal of Neuroscience Nursing
Pamela Newland, Mark P. Jensen, Chakra Budhathoki, Rebecca Lorenz
ABSTRACT
Purpose: The purpose of this study was to compare the rates of secondary health conditions in individuals with multiple sclerosis (MS) with age-matched U.S. general population norms.
Method: This was a cross-sectional study in which data were collected using a Web-based survey from members of the greater Midwest MS society chapter. Questions were modeled from the National Health Interview Survey to assess the presence of six health conditions. Self-reported health conditions among the sample were compared to U.S. general population norms from the National Health Interview Survey.
Results: Individuals with MS reported higher rates of depression, arthritis, diabetes, coronary artery disease, migraine headaches, and cancer than the normative population. Although the rates of health conditions increased with age in the normative sample, the MS sample showed a curvilinear (bimodal) pattern as a function of age for some secondary health conditions.
Multiple sclerosis (MS) is a chronic and often debilitating neurological disease that has its onset in early adulthood. Individuals with MS may experience a number of symptoms that can have a negative impact on overall health and quality of life (QOL; Newland, Naismith, & Ulione, 2009; Oleen-Burkey, Castelli-Haley, Lage, & Johnson, 2012). A diagnosis of MS has also been associated with the presence of other health conditions such as migraine headaches (Bigal & Lipton, 2008; Fromont et al., 2013), heart disease (Marrie et al., 2013; Motl, Fernhall, McAuley, & Cutter, 2011), stroke (Tortorella, Rocca, Colombo, Annovazzi, & Comi, 2006), and depression (Beiske et al., 2008; Thielscher, Thielscher, & Kostev, 2013). However, the rates of secondary health conditions and methods for recognizing these conditions in individuals with MS across age cohorts have not yet been well documented.
As individuals with MS age, they face many of the same age-related symptoms and secondary health conditions associated with aging in the general population (Alschuler, Ehde, & Jensen, 2013; Beiske et al., 2008; Marrie & Hanwell, 2013). However, research suggests that individuals with MS may have to deal with some of these conditions at younger ages than individuals who are aging without MS. For this reason, individuals with MS are said to ‘‘age faster’’ than those without MS (Molton et al., 2013, Rosenberg, Bombardier, Artherholt, Jensen, & Motl, 2013). The secondary health conditions that individuals with MS may develop as they age can also contribute to physical and mental problems, increased disability, and decreased overall QOL (Newland, WipkeTevis, Williams, Rantz, & Petroski, 2005).
One limitation to understanding the impact of aging on secondary health conditions in individuals with MS is the lack of comparisons to age-specific population norms on the frequency of these conditions. Such data would be useful for assessing the burden of disease at the population level, including the impact of the presence of health conditions on health services utilization and costs. The purpose of this study was to address this knowledge gap by comparing the rates of self-reported health conditions in individuals diagnosed with MS with age matched, U.S. population norms. Specifically, we used the National Health Interview Survey (NHIS; Centers for Disease Control and Prevention, 2012) questions to inquire about the presence of depression, coronary artery disease (CAD), migraine headaches, some forms of arthritis, cancer or other malignancy, or diabetes. We then compared the self-reported rate of these conditions overall and within specific age cohorts in our sample compared with NHIS data. On the basis of previous research, we hypothesized that the rates of health conditions in our sample of individuals with MS would be greater than those in the U.S. population norms. We did not have specific hypotheses regarding the patterns of rates of the conditions examined over different age cohorts because these have not been examined in the research literature. However, we were interested in determining if the pattern we expected to see in the normative population (i.e., an increase in the frequency of health conditions with age) would be replicated in the MS sample.
Study Design and Sample
This project used cross-sectional survey data obtained from 339 individuals with MS who were members of the local Gateway Chapter of the National MS Society email registry. The survey was deployed from February 24, 2012, to June 7, 2013. The Gateway Chapter MS society has a registry of more than 6,000 individuals who have MS; 1,952 of whom have Internet access. Individuals were included if they had Internet access, had a diagnosis of MS, and were at least 18 years old.
Procedure
The institutional review board of Southern Illinois University, Edwardsville, approved the study. An email notification describing the study was sent to the MS society email registry. The invitation email included a unique identifier that was linkable to the Qualtrics survey software and a link to a Web-based survey designed for this study. The survey was anonymous and without identifiers. The survey was designed using Qualtrics software of the Qualtrics Research Suite (Qualtrics Software Company, 2012; Provo, UT), a user-friendly interface compliant with the Health Insurance Portability and Accountability Act for collecting data in a secure environment.
Measures
Demographic Information
Participants were asked to provide information regarding age, gender, race/ethnicity, educational level, composition of household, household and individual income level, and time since self-reported symptom onset and actual diagnosis.
Health Conditions
Six questions from the NHIS relevant to individuals with MS were used to assess the presence of six health conditions. Each of the questions began with the phrase, ‘‘have you EVER been told by a doctor or other health professional that you hadI’’; this phrase was followed by a health condition (e.g., CAD, some form of arthritis, migraine headache, and diabetes [not including diabetes during pregnancy]).
These researchers set out to address the existing knowledge gap related to secondary health conditions in individuals with multiple sclerosis (MS) in comparison with age-matched, U.S. population norms.
Data Analysis 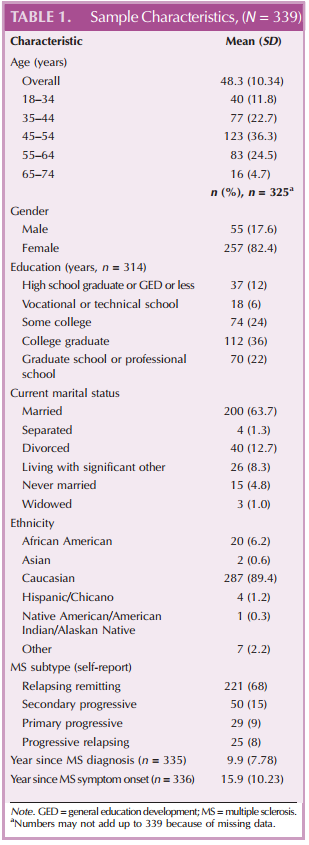
Data were first checked for completeness and quality. All available survey data were analyzed without imputation of missing values. We then computed descriptive statistics to summarize characteristics of the study sample. Continuous variables were summarized using number of observations, mean, and standard deviation. Categorical variables were summarized using count and percentage.
Next, we compared the rate of endorsement of each of the six health conditions in our sample with national norms using national adult survey data. Comparisons were made using a one-sided one-sample z test, under large sample assumption, with a national norm as a test value. We determined any difference between percentage as statistically significant if p G .05. Tests were performed for overall estimate of the sample as a whole as well as for the following specific age categories: 18Y34, 35Y44, 45Y54, 55Y64, and 65Y74 years. All the statistical analyses were performed using SPSS Version 20 (IBM Corp., Armonk, NY).
Results
Sample Description Three hundred sixty-nine online surveys were sent via email link to potential participants with MS, and 339 were completed (completion rate = 92%). Most of the study participants were Caucasian (92%) and women (77%). Mean age at MS symptom onset was 48.3 years (SD = 10.34 years). Demographic and clinically related data are presented for the study sample (Table 1).
Rates of Health Conditions
The most commonly reported secondary health conditions in the sample were depression, migraine headaches, arthritis, CAD, diabetes, and cancer or malignancies (Table 2). The results comparing the rates of these conditions in our sample with the U.S. population indicated that the percentage of depression, migraine headache, some forms of arthritis, and cancer were more prevalent in our sample (Table 2). The z tests and corresponding 95% confidence intervals showed that depression was significantly higher in percentage in all age cohort groups (55% vs. national norm of 3% with a 95% confidence interval [46%, 57%] for the difference,z = 18.5, p G .0001).
Likewise, migraine headaches (37% vs. national norm of 17% with a 95% confidence interval [15%, 25%] for the difference, z = 7.4, p G .0001) and arthritis (32% vs. national norm of 25% with a 95% confidence interval [2%, 12%] for the difference, z = 2.7, p = .003) were significantly higher in the study sample than the national norms. Among those in the younger (18Y34 years) and middle-age (35Y44 and 45Y54 years) groups, migraines were significantly more common, and there was higher percentage of CAD in the middleage group (35Y44 years) in our sample, relative to the U.S. normative sample.
Although the changes with age were similar between the MS sample and norms for cancer (increasing with age), migraine (evidencing higher rates in younger cohorts), and arthritis (increasing with age), there were differences in the pattern of age effects between the sample and norms for other conditions (Fig 1). For example, although the occurrence of CAD increased with increasing age in the normative sample, it evidenced a curvilinear relationship with age in the MS sample, with a relatively high rate in the 35- to 44-year-old cohort, a decrease in frequency in the 45- to 54-year-old cohort, and an increase in frequency with each subsequent age cohort. Diabetes showed a similar pattern in the MS sample, with its first peak (in frequency) in the 35- to 44-year age cohort, a subsequent decrease in frequency, and an increasing frequency with age from there. In the normative sample, depression increased with age to late middle age (55Y64 years) and then evidenced a decrease in frequency. In the MS sample, depression was most common in the youngest age cohort (18Y34 years) and least common in the young adults (35Y44 years), peaking again in late middle age (55Y64 years). Depression rate was significantly higher in the MS sample than the national estimate for each age category. Unlike the other health conditions, diabetes was not significantly more common in the MS sample, relative to the normative sample.
Discussion 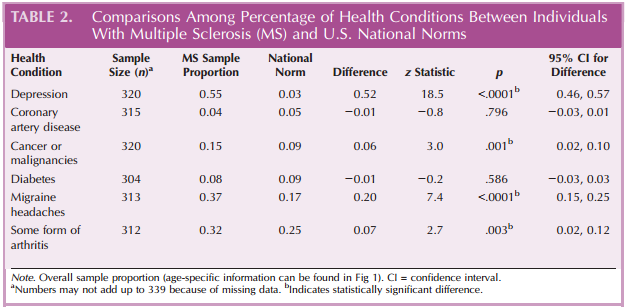
The study findings indicate that the rates of individuals with depression, CAD, migraine headaches, and some forms of arthritis are higher in individuals with MS than in the U.S. norms. Collectively, these findings indicate that individuals who have been diagnosed with MS for over 3 years have more secondary health conditions than the general population and that the secondary health conditions may occur at different ages for individuals with MS. It is striking to note that the frequency of migraine headaches decreases with age in both our sample and in the normative sample, whereas the frequencies of cancer and arthritis increase with age in both groups.
On the other hand, a curvilinear association between age and the frequency of CAD and diabetes (e.g., more common in age groups of 35Y44 and 65Y74 years, respectively) was found in our sample, and this finding was not evident in the normative group. Although not statistically significant, this is important clinical information for healthcare providers who care for individuals with MS. Problems with CAD may be a potential precursor of additional health decline among those who are 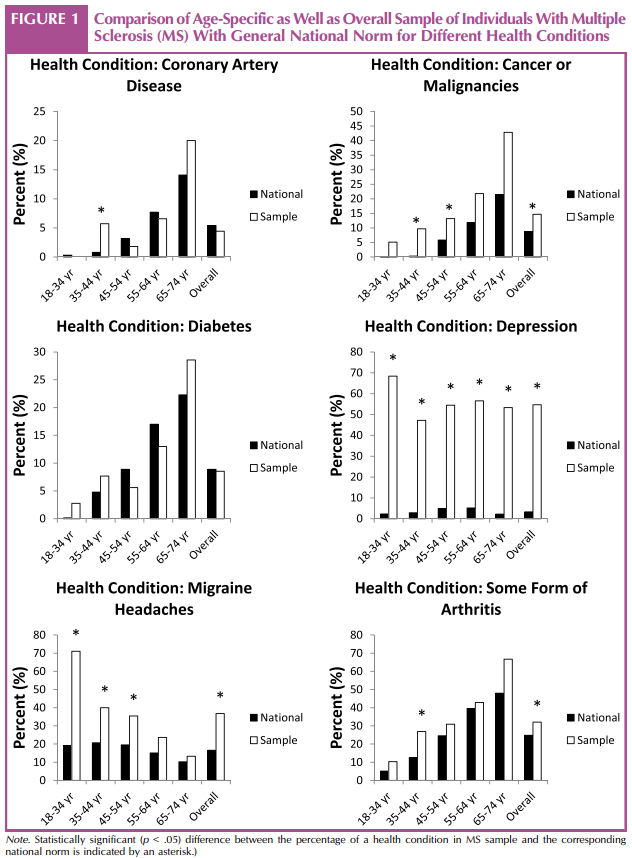 younger and may reflect accelerated aging. Thus, those who have CAD when they are younger tend to have subsequent increases in morbidity and mortality, whereas having a diagnosis of CAD later in life does not tend to be strongly linked to the development of other health conditions (Grytten Torkildsen, Lie, Aarseth, Nyland, & Myhr, 2008). In contrast, diabetes may have different implications as a function of age at onset of diagnosis. Among younger individuals, the steps required to manage the condition might be viewed as having significant negative impacts on their lifestyle and may therefore result in more distress or even greater risk for poor management. Older individuals with MS, on the other hand, may view the requirements of diabetes management as less of an intrusion on their lifestyle and therefore cope with the disease better than someone who is younger (Mozaffarian et al., 2009).
younger and may reflect accelerated aging. Thus, those who have CAD when they are younger tend to have subsequent increases in morbidity and mortality, whereas having a diagnosis of CAD later in life does not tend to be strongly linked to the development of other health conditions (Grytten Torkildsen, Lie, Aarseth, Nyland, & Myhr, 2008). In contrast, diabetes may have different implications as a function of age at onset of diagnosis. Among younger individuals, the steps required to manage the condition might be viewed as having significant negative impacts on their lifestyle and may therefore result in more distress or even greater risk for poor management. Older individuals with MS, on the other hand, may view the requirements of diabetes management as less of an intrusion on their lifestyle and therefore cope with the disease better than someone who is younger (Mozaffarian et al., 2009).
Depression was common in our sample and occurred at higher rates across all age cohorts, relative to the U.S. norms. This finding is consistent with a number of other studies of depression in individuals with MS (Beiske et al., 2008; Marrie et al., 2013; Thielscher et al., 2013). The potential MS-specific causes of depression can include factors associated with living with a chronic illness as well as the adverse effects of some medications (Oliver-Quetglas, Torres, March Socias, & Esteva, 2013).
Of note, the younger age group (18Y34 years) in our sample reported the highest frequency of depression. This suggests that depression is not necessarily related to living for many years with a chronic disease (Alschuler et al., 2013; Benedict et al., 2013; Rosenberg et al., 2013; Thielscher et al., 2013). In fact, just the opposite may be true:V The longer one lives with a chronic disease such as MS, the more one might learn strategies to adapt and cope with the symptoms and disability. This finding is consistent with previous research regarding depression in individuals with other chronic illness (Oliver-Quetglas et al., 2013). The finding also suggests that depression may be connected with having a recent diagnosis of MS, the start-up of new medications, social pressures, and perhaps, day-to-day work and family responsibilities in the younger age group. Prospective research with age-matched individuals is needed to better understand the (preventable) causes of depression in younger individuals with MS, because this information can be used to help develop interventions to prevent and limit the negative impact of depression in these individuals.
Our findings also indicate that individuals with MS endorse a diagnosis of migraine headaches more often than the general U.S. population. This higher rate of migraine was particularly evident in the middle-age and older cohorts (35Y44, 45Y54, and 55Y64 years). These findings are consistent with others who report that twice as many individuals with MS report migraine headaches compared with controls (Bible, 2013; Bigal & Lipton, 2008; Lin, Wang, Chiang, Peng, & Yang, 2013).
The reason for these relatively high rates of migraines in the younger group of our MS sample is not yet entirely clear. One possible factor may be the lesion location in MS (Benedict et al., 2013; Oliver-Quetglas et al., 2013). The importance of lesion location has been suggested after observations that lesions within the midbrain are more commonly associated with migraine than lesions at other locations in individuals with MS. The age-related effects on the rates of migraine in our sample may be related to the possibility that onset of migraine is seen at a younger age in MS populations. Certainly, others have noted that migraines tend to occur less frequently in older individuals with MS (Bible, 2013; Schramm et al., 2013). In any case, given the frequency of migraine in younger individuals with MS, headache could play a significant role in MS disease trajectory. These are explanations that require additional exploration.
Our findings, as well as those of others (Cooper, Bynum, & Somers, 2009; Marrie & Hanwell; 2013; Somers, Thomas, Smeeth, & Hall, 2009), reveal that co-occurring autoimmune diseases have been observed within individuals with MS and rheumatoid arthritis. The reasons for this association are not entirely clear. Interestingly, there is emerging evidence of genetic similarities between these two autoimmune disorders (Somers et al., 2009). Researchers have also found that certain health conditions (e.g., psychiatric disorders and diabetes) are more commonly reported among an older age cohort with MS than other chronic conditions (Fromont et al., 2013; Marrie et al., 2013). The process of aging along with the common accumulation of secondary health conditions may create difficulty in teasing out relationships.
Limitations
An important limitation of the current study is the use of cross-sectional data, which limits our ability to draw inferences regarding the causal effects of age on the occurrence of the health conditions assessed. Longitudinal research is needed to help tease out the natural course and predictors of the development of health conditions over time. Although the use of the NHIS questions in our survey made it possible to perform direct comparisons with national norms, the precision of the estimates in our sample was limited by use of self report and the limited number of surveys totally completed by individuals in each age cohort. Despite an attempt to send out additional emails for the study survey, we did not accrue a larger, representative sample of participants from the local MS Society database. Finally, our sample was limited to the greater Midwest area and therefore does not necessarily represent individuals with MS as a whole. Additional research using other samples of individuals with MS is needed to determine the generalizability of our findings.
Recommendations for Future Research
The findings indicate that more research studying age effects on secondary health conditions in individuals with MS is warranted. Longitudinal studies and replication of these findings should be performed to strengthen generalizability. More research is also needed to determine the specific negative impact of health conditions in individuals with MS as they age. Such research could provide an empirical basis for the development of evidenced-based interventions that would enhance the overall health and QOL of individuals with MS.
Conclusions and Implications for Nursing Practice
Our analyses present comparisons of common health conditions in individuals with MS compared with a U.S. population. We found that individuals with MS reported significantly higher rates of depression, migraine, and some forms of arthritis, relative to the general U.S. population. Likewise, although not statistically significant, our older age group reported higher rates of other secondary health conditions (e.g., CAD and diabetes) compared with the U.S population. Our results also indicate an aging effect on the frequency of health conditions and that the pattern of this effect in individuals with MS may be sometimes similar to those in the normative population (i.e., increasing with age) and sometimes may show a curvilinear association (i.e., bimodal distribution). Individuals with MS not only are at greater risk than the general population for having a number of comorbid health conditions but also, for some conditions, may be at an even greater risk at a younger age. Such findings are relevant for nurses who care for individuals with MS to recognize and prevent the development of secondary health conditions. The potential benefits of age-specific, targeted approaches for depression, CAD, migraine, and arthritis should be part of routine nursing care.
Acknowledgment
The authors thank the Gateway Chapter of the National MS Society.
REFERENCES
Alschuler, K. N., Ehde, D. M., & Jensen, M. P. (2013). The cooccurrence of pain and depression in adults with multiple sclerosis. Archives of Physical Medicine and Rehabilitation, 94, 731Y736. doi:10.1016/j.apmr.2012.11.014. Epub 2012 Nov 16.
Beiske, A. G., Svensson, E., Sandanger, I., Czujko, B., Pedersen, E. D., Aarseth, J. H., & Myhr, K. M. (2008). Depression and anxiety amongst multiple sclerosis patients. European Journal of Neurology, 15, 239Y245.
Benedict, R. H., Schwartz, C. E., Duberstein, P., Healy, B., Hoogs, M., Bergsland, N., I Zivadinov, R. (2013). Influence of personality on the relationship between gray matter volume and neuropsychiatric symptoms in multiple sclerosis. Psychosomatic Medicine, 75(3), 253Y261.
Bible, E. (2013). Pain: Comorbidity of neuropathic pain and migraine in patients with multiple sclerosis. Nature Reviews Neurology, 9, 544. doi:10.1038/nrneurol.2013.175
Bigal, M. E., & Lipton, R. B. (2008) Concepts and mechanisms of migraine chronification. Headache, 48, 7Y15.
Centers for Disease Control and Prevention. (2012). About the National Health Interview Survey Retrieved from http://www .cdc.gov/nchs/nhis/about_nhis.htm
Cooper, G. S., Bynum, M. L., & Somers, E. C. (2009). Recent insights in the epidemiology of autoimmune diseases: Improved prevalence estimates and understanding of clustering of diseases. Journal of Autoimmunity, 33, 197Y207. doi:10.1016/j.jaut.2009.09.008
Fromont, A., Binquet, C., Rollot, F., Despalins, R., Weill, A., Clerc, L., I Moreau, T. (2013). Comorbidities at multiple sclerosis diagnosis. Journal of Neurology, 260, 2629Y2637.
Grytten Torkildsen, N., Lie, S. A., Aarseth, J. H., Nyland, H., & Myhr, K. M. (2008). Survival and cause of death in multiple sclerosis: Results from a 50-year follow-up in Western Norway. Multiple Sclerosis, 14(9), 1191Y1198. doi:10.1177/1352458508093890
Lin, G. Y., Wang, C. W., Chiang, T. T., Peng, G. S., & Yang, F. C. (2013). Multiple sclerosis Presenting initially with a worsening of migraine symptoms. Journal of Headache Pain, 14(1), 70. doi:10.1186/1129-2377-14-70
Marrie, R. A., Fisk, J. D., Yu, B., Leung, S., Elliott, L., Caetano, P., I CIHR Team in the Epidemiology and Impact of Comorbidity on Multiple Sclerosis. (2013). Mental comorbidity and multiple sclerosis: Validating administrative data to support population based surveillance. BioMedCentral Neurology, 13, 16.
Marrie, R. A., & Hanwell, H. (2013). General health issues in multiple sclerosis: Comorbidities, secondary conditions, and health behaviors. Continuum, 19, 1046Y1057. doi:10.1212/ 01.CON.0000433284.07844.6b
Molton, I., Cook, K. F., Smith, A. E., Amtmann, D., Chen, W. H., & Jensen, M. P. (2013). Prevalence and impact of pain in adults aging with a physical disability: Comparison to a US general population sample. Clinical Journal of Pain, 30, 307Y315.
Motl, R. W., Fernhall, B., McAuley, E., & Cutter, G. (2011). Physical activity and self-reported cardiovascular comorbidities in individuals with multiple sclerosis: Evidence from a crosssectional analysis. Neuroepidemiology, 36, 183Y191. doi:10 .1159/000327749
Mozaffarian, D., Kamineni, A., Carnethon, M., Djouss2, L., Mukamal, K. J., & Siscovick, D. (2009). Lifestyle risk factors and new-onset diabetes mellitus in older adults: The cardiovascular health study. Archives of Internal Medicine, 169(8), 798Y807.
Newland, P. K., Naismith, R. T., & Ullione, M. (2009). The impact of pain and other symptoms on quality of life in women with relapsing-remitting multiple sclerosis. Journal of Neuroscience Nursing, 41, 322Y328.
Newland, P. K., Wipke-Tevis, D. D., Williams, D. A., Rantz, M. J., & Petroski, G. F. (2005). Impact of pain on outcomes in longterm care residents with and without multiple sclerosis. Journal of the American Geriatric Society, 53, 1490Y1496.
Oleen-Burkey, M. A., Castelli-Haley, J., Lage, M. J., & Johnson, K. P. (2012). Burden of a multiple sclerosis relapse: The patient’s perspective. Patient, 5, 57Y69.
Oliver-Quetglas, A., Torres, E., March, S., Socias, I. M., Esteva, M. (2013). Risk factors of depressive syndrome in young adults. Actas Espan˜olas de Psiquiatrı´a, 41, 84Y86.
Qualtrics Software Company. (2012). Qualtrics software of the Qualtrics Research Suite. Provo, UT: Author.
Rosenberg, D. E., Bombardier, C. H., Artherholt, S., Jensen, M. P., & Motl, R. W. (2013). Self-reported depression and physical activity in adults with mobility impairments. Archives of Physical Medicine and Rehabilitation, 94, 731Y736. doi:10.1016/j.apmr .2012.11.014
Schramm, S. H., Oberman, M., Katsarava, Z., Diener, H. C., Moebus, S., & Yoon, M. S. (2013). Epidemiological profiles of patients with chronic migraine and chronic tension-type headache. Journal of Headache Pain, 14, 40. doi:10.1186/ 1129-2377-14-40
Somers, E. C., Thomas, S. L., Smeeth, L., & Hall, A. J. (2009). Are individuals with an autoimmune disease at higher risk of a second autoimmune disorder? American Journal of Epidemiology, 169, 749Y755. doi:10.1093/aje/kwn408
Thielscher, C., Thielscher, S., & Kostev, K. (2013). The risk of developing depression when suffering from neurological diseases. German Medical Science, 11. doi:10.3205/000170
Tortorella, P., Rocca, M. A., Colombo, B., Annovazzi, P., Comi, G., & Filippi, M. (2006). Assessment of MRI abnormalities of the brainstem from patients with migraine and multiple sclerosis. Journal of Neurological Sciences, 244(1Y2), 137Y141.