Management of Multiple Sclerosis During Pregnancy and the Reproductive Years

Selected By
Megan Weigel, DNP, ARNP-c, MSCN
Why is this important to me?
Because MS affects many women during their childbearing years, reproductive issues are important for many women with the disease. Although in previous years women with MS were discouraged from becoming pregnant, doctors now know that most women with MS can have a successful, healthy pregnancy, and health care professionals generally encourage and support women with MS who wish to have a baby. This article reviews many aspects of pregnancy that are important to ensure optimal management of MS and health of the baby.
What is the objective of this study?
The following should be considered if you have MS and are thinking about becoming pregnant:
- About one-half of pregnancies are unplanned. If you are a woman with MS of reproductive age, it is important that you continue to seek family planning counseling.
- The use of oral contraceptives (birth control pill) may be beneficial in MS, but study results are conflicting.
- Most doctors recommend that you discontinue your MS medication prior to becoming pregnant and that you allow 2-6 weeks for the drug to be cleared from your system before trying to conceive. If your MS is active or highly active, you may be able to switch to glatiramer acetate because the benefits may outweigh the risks. The use of intravenous immunoglobulin or steroids may be useful in women with high MS disease activity who are past the first trimester. Use of these agents may also help prevent relapses after delivery.
- No differences in fertility or the use of assisted reproductive technology (in vitro fertilization, etc.) have been reported in women with MS compared to the general population. Some studies have reported an increased relapse rate if using assisted reproductive technology, but factors that may independently impact MS such as discontinuing medication and emotional stress were not assessed. You should not hesitate to discuss your plans with your healthcare provider.
- The impact of pregnancy and delivery on relapse rates is unclear.You may experience a decreased rate of relapse during pregnancy, especially during the last trimester. You may experience an increased rate of relapse during the first 3 months after giving birth. Other studies show that pregnancy has a beneficial effect on relapses and disability. Researchers continue to explore the effects of pregnancy on relapse rates during and after delivery and long-term outcomes of MS.
- MRI during pregnancy appears to be safe, but contrast agents containing gadolinium should generally be avoided while pregnant.
- The choice of delivery method (vaginal or Cesarean) and the choice of delivery anesthesia are determined by your obstetrical needs and not your MS. Anesthesia choices appear to have no impact on MS relapses or disease progression.
- Having MS does not appear to increase the risk of miscarriage, stillbirth, or birth defects.
- Children born to a woman with MS have a relatively low absolute risk of developing MS later in life.
- For breastfeeding mothers, resumption of MS medications is typically delayed until the baby is weaned. Breastfeeding,especially exclusive breast-feeding, may provide some protection against relapses.
- Your healthcare professional should screen you for depression after delivery.
The decision to start a family is an important one. Involving your healthcare provider early in your planning can help to ensure a good outcome for your baby and your disease management.
How did the authors study this issue?
The authors reviewed published studies and clinical trials that investigated the relationship between MS and various aspects of pregnancy.
Original Article
Management of Multiple Sclerosis During Pregnancy and the Reproductive Years
A Systematic Review
Obstetrics & Gynecology
Bove, Riley MD, MMSc; Alwan, Sura PhD; Friedman, Jan M. MD, PhD; Hellwig, Kerstin MD; Houtchens, Maria MD, MMSc; Koren, Gideon MD; Lu, Ellen PhD; McElrath, Thomas F. MD, PhD; Smyth, Penelope MD; Tremlett, Helen PhD; Sadovnick, A. Dessa PhD
Abstract
OBJECTIVE: To examine the evidence guiding management of multiple sclerosis (MS) in reproductive-aged women.
DATA SOURCES: We conducted an electronic literature search using PubMed, ClinicalTrials.gov, and other available resources. The following keywords were used: “multiple sclerosis” and “pregnancy.” We manually searched the reference lists of identified studies.
METHODS OF STUDY SELECTION: Two reviewers categorized all studies identified in the search by management topic, including effect of pregnancy on MS course, fetal risks associated with disease-modifying treatments during pregnancy, and management of patients off disease-modifying treatment. We categorized studies by strength of evidence and included prior meta-analyses and systematic studies. These studies were then summarized and discussed by an expert multidisciplinary team.
TABULATION, INTEGRATION, AND RESULTS: The risk of MS relapses is decreased during pregnancy and increased postpartum. Data are lacking regarding the risks of disease-modifying treatments during pregnancy. There may be an increased risk of MS relapses after use of assisted reproductive techniques. There does not appear to be a major increase in adverse outcomes in newborns of mothers with MS.
CONCLUSION: Although there are many unmet research needs, the reviewed data support the conclusion that in the majority of cases, women with MS can safely choose to become pregnant, give birth, and breastfeed children. Clinical management should be individualized to optimize both the mother's reproductive outcomes and MS course.
Multiple sclerosis (MS) is a chronic inflammatory disorder of the central nervous system, primarily affecting white matter in the brain and spinal cord. The principal pathologic features of MS are autoimmune destruction of myelin and subsequent axonal degeneration. Clinical deficits are manifested in a number of functional systems (fatigue, cognition, mood, vision, ambulation, dexterity, sensation, bladder and bowel function). Initially, MS is often characterized by a relapsing-remitting course with over time a decline in relapses but an accelerated progression of disability (secondary progressive).
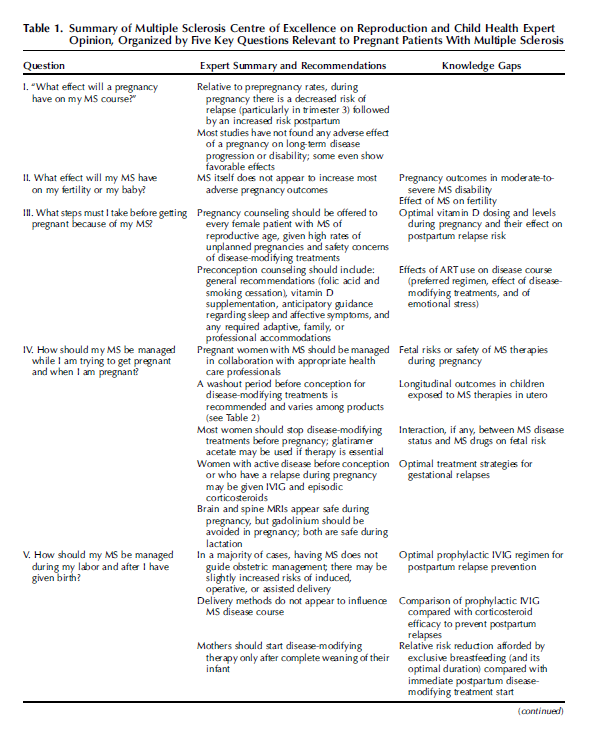
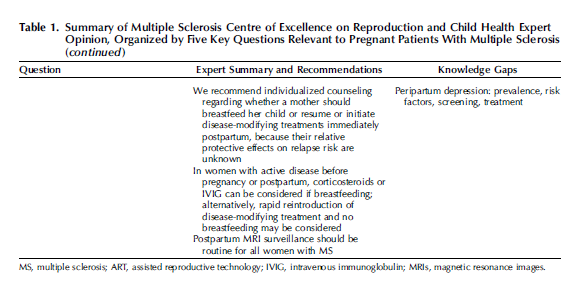
Multiple sclerosis preferentially affects females, with clinical onset often during childbearing years; hence, reproduction is an important consideration for many women with MS. Although MS specialists often advised against childbearing previously, today health care professionals are supporting young adults with MS in raising families. The Multiple Sclerosis Centre of Excellence on Reproduction and Child Health (MS-CERCH) is an international collaborative multidisciplinary research consortium that emerged in response to an increasing need for evidence-based, up-to-date information around childbearing in MS. Our mandate is to provide evidence-based strategies in reproductive decision-making to individuals with MS and their health care providers. We review and evaluate the available literature, highlight knowledge gaps, and provide consensus recommendations on the management of reproduction in MS.
SOURCES
We performed a comprehensive literature review around management of MS in women before, during, and after pregnancy. Evidence was gathered primarily through a search of PubMed, Embase, ClinicalTrials.gov, and other resources with the final search completed on August 12, 2014.
STUDY SELECTION
Study selection included all English-language papers combining the keywords “pregnancy” and “multiple sclerosis” for all years available from each database. Reference lists of identified articles were searched for further manuscripts. Two reviewers categorized studies by management topic (Table 1) and strength of evidence. Most studies were observational; few were prospective, and fewer were randomized interventional studies. We also included meta-analyses and systematic studies. The entire MS-CERCH team then discussed individual study merits and limitations and made consensus recommendations, evidenced-based where possible, but primarily consisting of expert opinion.
RESULTS
When planning a pregnancy, important counseling and management considerations for women with MS include both effects of pregnancy on MS and effects of MS on fertility, genetic counseling, and preconception care including discontinuation of MS therapies. Because up to 50% of pregnancies may be unintentional, all women with MS of reproductive age should be counseled at each clinical encounter to ensure adequate reproductive planning. Whenever possible, we advise face-to-face, individualized preconception counseling; online childbearing resources are underexplored in MS.
The best studied aspect of childbearing in MS is the effect of pregnancy on relapse risk. According to the American Academy of Neurology's criteria for prognostic questions, the evidence is “moderate” for a decreased relapse rate during pregnancy (notably during the third trimester) and “moderate to strong” for an increased relapse rate postpartum relative to prepregnancy rates. In the first 3 months postpartum, up to 30% of women may relapse, and relapses may worsen long-term disability. Over the whole prepregnancy to postpregnancy period, the relapse risk appears to be similar to the nonpregnant state. Small observational imaging studies demonstrating increased inflammatory activity corroborate clinical reports. The increase in relapses postpartum coincides with dramatic hormonal shifts and loss of the immunotolerant state of pregnancy; the most studied of these is the rapid postpartum decline of estriol levels. Factors associated with but not necessarily predictive of postpartum relapses include high relapse rate in the prepregnancy year and during pregnancy and a higher disability level at conception.
Pregnancy reportedly has either no adverse effects on maternal MS progression and disability or a beneficial effect. Important confounders often overlooked in studies include reverse causation, whereby women with more severe disease are less likely to have children, and age at MS onset. Maternal age appeared to fully explain delay in disability progression in one large study but not in three others.
Fertility in women with MS could be affected by reproductive decision-making, decreased libido or sexual function, lower estrogen levels, thyroid autoimmunity, temporary therapy-related amenorrhea, or premature ovarian failure. Nevertheless, no reliable studies have demonstrated altered rates of fertility or use of assisted reproductive technology in women with MS. We encourage women to consider strategies (eg, ovulation predictors, fertility consultations) to increase the chance of conceiving while they are relatively healthy and not on any disease-modifying treatment.
Assistive reproductive technology accounts for at least 1% of live births in developed countries, and an increased MS relapse risk has been reported after assisted reproductive technology; this was most tied to unsuccessful cycles, and to ovulation stimulation with gonadotropin-releasing hormone agonists rather than antagonists. Confounding from timing of MS treatment interruption and emotional stressors has not been assessed. Dialogue between obstetric and neurologic teams is essential before assisted reproductive technology cycles.
Oral contraceptive use may be mildly protective for MS onset or course, but studies are conflicting and may be confounded by the effect of oral contraceptives on delaying childbearing. Interaction studies between oral contraceptives and disease-modifying treatments are limited, and no MS-specific considerations in the choice of oral contraceptive are reported. Women discontinuing oral contraceptives for a pregnancy may be advised to use mechanical contraception and continue on their MS treatment until fully ovulatory to avoid prolonged treatment interruption.
In addition to routinely recommended prenatal vitamins and 0.4–1.0 g daily of folic acid,74 MS-specific preconception considerations include smoking cessation as a result of a possible role in disease progression, sleep hygiene counseling, and vitamin D supplementation. Optimal dosing of vitamin D during pregnancy remains unknown: supranormal serum levels should be avoided, and 1,000–2,000 IU daily is believed to be safe.
Women may be concerned about risk of transmission of MS to their children. Multiple sclerosis is associated with environmental and genetic risk factors with a complex genetic pattern with more than 100 genetic susceptibility loci identified.88 Children born to a woman with MS have a 20–50 times increased risk of developing MS compared with the general population, but the absolute risk is relatively low (3–5%). Children born to parents who both have MS have a greater than 20% risk of developing MS later in life. Predictive testing is not available for MS.
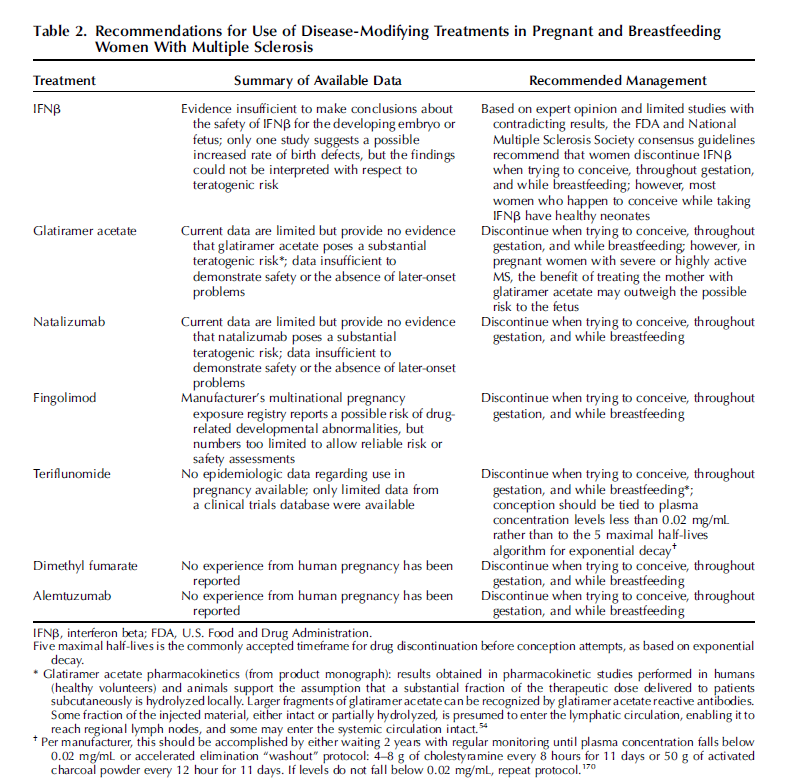
Opinions vary on disease-modifying treatment use while trying to conceive, but most clinicians recommend discontinuation. Disease-modifying treatments reduce the frequency of exacerbations in relapsing forms of MS but are not effective for treating acute relapses. The currently approved first-line disease-modifying treatments are listed in Table 1. Alemtuzumab has also been approved in some jurisdictions. Because disease-modifying treatments are biologically and chemically diverse, it is unlikely that they would all affect the developing embryo or fetus in the same way. Although the results of limited studies in pregnant women to date have generally been reassuring, and no disease-modifying treatment is known to be teratogenic in humans (Appendix 1, available online at http://links.lww.com/AOG/A570), larger studies are needed to assess the reproductive toxicity of individual treatments. The large molecular size of some biologic therapies may limit transfer across the placenta before 20 weeks of gestation, although active transport may occur after that time. Other effects of gestational exposure including on the placenta are possible; long-term sequelae have not been evaluated. Table 2 summarizes our recommendations for use of disease-modifying treatments during pregnancy. In general, five maximal half-lives is the commonly accepted timeframe for drug discontinuation before conception based on exponential decay. Typically, this represents a 2- to 6-week timeframe.
Other immunologic treatments, not always licensed for but which are occasionally used in MS, are contraindicated during pregnancy and should be discontinued before conception (Appendix 2, available online at http://links.lww.com/AOG/A570). Among these, rituximab is an anti-CD20 monoclonal antibody whose use in MS is increasing; its teratogenic risk is undetermined.
A pregnancy test should be considered before prescribing any MS treatment (including infusions). Some symptomatic medications may be continued while trying to conceive, following standard guidelines for safety in pregnancy.
For pregnant women with severe or highly active MS, the benefit of MS treatment may outweigh the (unknown) risk to the fetus. If such treatment is necessary, clinicians may consider switching to a different drug such as glatiramer acetate U.S. Food and Drug Administration Category B (Appendix 1, http://links.lww.com/AOG/A570).
Achieving a pregnancy may take some time so discontinuation of disease-modifying treatment during this period may increase relapse risk. Women who are perceived to be at high risk for a relapse (eg, rebound relapse after discontinuation of certain treatments) or those who have a history of delayed conception may need monthly intravenous corticosteroids, usually at the start of menses with a negative pregnancy test, until conception occurs.
Once a woman with MS is pregnant, prevention of relapses can be an overriding consideration if there was high disease activity before pregnancy. Either monthly intravenous immunoglobulin (IVIG) or monthly steroids after the first trimester can be considered, but safety data are limited. Corticosteroid use should be limited if possible throughout pregnancy. An increased risk of cleft lip and palate among the neonates was reported in several older studies with corticosteroid use in the first trimester, but not in a more recent study. In the second and third trimesters, use has been associated with low birth weight and possibly premature delivery, although these findings may be confounded by the underlying disease. Less than 10% of the maternal dose of prednisone, prednisolone, and methylprednisolone reaches the fetus as a result of metabolism to inactive forms by the placenta; unfortunately, the potential teratogenic effect of these inactive forms is uncertain. In contrast, betamethasone and dexamethasone do cross the placenta with minimal metabolism. Thus, the full adult dose likely reaches the fetus, and these should never be used outside of the brief obstetric indication of promoting fetal lung maturity. Treatment of a serious MS relapse typically consists of either IVIG or intravenous corticosteroids with the same risks outlined previously.
There is no evidence that magnetic resonance imaging exposure up to 3 Tesla is associated with fetal harm during pregnancy, but gadolinium should only be used if it is likely to change management and benefit the patient or fetus. Written informed consent is recommended by the American College of Radiologists to document patients' understanding of risk. With respect to lactation, the excretion of both gadolinium-based and iodinated contrast agents into breast milk is low, as is their absorption from the infant gut. Thus, the use of contrast agents in the mother is considered safe during lactation without the need to interrupt breastfeeding.
At delivery, obstetric indications guide the mode of delivery for patients with most MS. Mothers with MS are often older than mothers in the general population because the typical age of MS onset is 30 years. Even when studies took into consideration maternal age, mothers with MS were reported as having a slightly increased risk of induction (which may be associated with higher disease severity), slower progression of second stage of labor, and increased use of forceps or operative delivery in comparison with women in the general population in most studies but not all. Rarely, severely disabled patients may be unable to push in the second stage of labor. A trend for increased cesarean or assisted vaginal delivery has been reported with increased MS disability as well as in some geographic regions.vWhether this is an effect of the disease, of women with severe disease choosing not to deliver vaginally, or of physicians' propensity to deliver patients with MS perceived as being at “high risk” in a more conservative fashion has not been adequately assessed.
The choice of obstetric anesthesia for women with MS typically depends on the mode of delivery. Multiparous women with MS were found to be more likely to receive epidural rather than spinal anesthesia compared with multiparous women in the general population. In addition, an increased duration of hospitalization for delivery and newborn care for women with MS, noted in previous studies, was not confirmed in a more recent one.
There is no measurable negative effect of obstetric anesthesia or of anesthesia type during delivery on postpartum relapses or disability progression despite anecdotal reports and historical opinion.
In terms of fetal outcomes, MS does not appear to increase the risk of early trimester pregnancy loss, stillbirth, or fetal malformation in most studies. There are some reports that mothers with MS may be more likely to have fetuses with reduced birth weight for gestational age but not specifically fetal growth restriction. The finding of reduced birth weight remains controversial, and potential causes are unknown.For instance, a study that reported significantly lower mean birth weight at term in mothers with an MS diagnosis compared with mothers who gave birth before MS onset failed to adjust for potential confounders. The largest study to date to assess the effect of MS on birth weights and on preterm birth rates (less than 37 weeks of gestation) was also the only to adjust for confounders (eg, multiple births to individual mothers, parity, hypertension, and prior preterm births). In contrast to smaller studies, no association was noted between MS status and either newborn birth weight or gestational age.
The biggest management question in the postpartum period is whether women with MS should resume their MS treatment or breastfeed. In addition to the known benefits of lactation for both infants and mothers, reflected in the World Health Organization recommendations of exclusive breastfeeding for 6 months,additional considerations in MS include the relative protection against postpartum relapses afforded by breastfeeding compared with early resumption of disease-modifying treatments.
Studies of exclusive breastfeeding have reported a protective effect of lactation on risk of postpartum relapses, whereas studies collapsing exclusive and nonexclusive breastfeeding have found no apparent protective effect. In a meta-analysis of these small studies, any breastfeeding reduced the risk of postpartum relapses by half. Disease activity, which can alter a patient's decision to breastfeed or restart disease-modifying treatment, may confound the association between breastfeeding and postpartum relapses. At least in a pilot study, vitamin D levels associated with breastfeeding did not appear to be a confounder.
The information available on the safety of disease-modifying treatments during lactation is limited. Breastfeeding is considered “moderately safe” for glatiramer acetate and interferon-[beta], where high molecular weight limits transfer into breast milk, and for natalizumab, despite reports that it is excreted into human breast milk. Information on breastfeeding during maternal use of other disease-modifying treatments is lacking.In light of limited evidence, women should resume MS treatments only after their infant is weaned from breast milk. In these patients, exclusive breastfeeding for 6 months should be supported if disease activity and fatigue permit, and postpartum surveillance magnetic resonance imaging with gadolinium should be used to monitor subclinical MS activity and guide earlier treatment resumption.
For breastfeeding mothers, options for relapse prevention or treatment include corticosteroids or IVIG. Monthly intravenous corticosteroids have been used to reduce the risk of postpartum relapses. Maternal corticosteroid treatment is generally believed to be safe for the infant ; small to moderate doses of corticosteroids ingested from milk add, at most, 10% to the infant's endogenous corticosteroid production and may be of little clinical significance. Nonetheless, because corticosteroids could lead to adverse events (eg, growth restriction) in children, combined with the much larger maternal doses used to treat relapses, suspending breastfeeding for 4 hours after infusion with a “pump and dump” approach is prudent. Prophylactic IVIG use during lactation has been examined in several studies and found to decrease the postpartum relapse rate in mothers. Differing protocols have been implemented, but an optimal dosing regimen that maximizes maternal MS benefit while moderating the high expense of IVIG has not been established; these include a double-blind, randomized trial (n=168 100) and a case series of IVIG (n=43) given within 3 days of delivery and then monthly. Maternal IVIG treatment does not seem to have adverse effects on the infant 100,101,103,136 with only a transient rash possibly caused by IVIG reported.
Multiple sclerosis-specific postpartum counseling should include discussion of potential triggers for MS exacerbations or symptom worsening. Strategies include minimization of sleep disruption (eg, scheduled naps during the day, pumping and storing breast milk on a schedule for others to feed to the baby while the mother naps) and help with household duties when available. Physical therapy may assist with resuming activity. Urologic symptoms may require evaluation to distinguish demyelinating from obstetric etiologies. Although of uncertain significance, thyroid antibodies appear to be elevated in mothers with MS postpartum.
It is estimated that 13–19% of all women experience depression in the first 6 months after delivery with the strongest risk factors being prior depression, stressful life events, and poor marital or social support. Women with MS would be expected to experience some exacerbation of affective symptoms peripartum given their increased baseline risk of mood disorders compounded by MS symptoms. Strategies to prepare the mother should be discussed early (with continuation of antidepressant drug therapy during pregnancy weighed against the known risks, like in pregnant women without MS ). We recommend that any health care professional caring for postpartum women with MS screen for depression. The use of screening tools (eg, Edinburgh Postnatal Depression Scale ) and the relative therapeutic benefits of antidepressant medications and nonpharmacologic interventions have not been assessed in MS.
CONCLUSIONS
Our recommendations for medical management of pregnant and other reproductive-aged women with MS are summarized in Table 1. Because the rate of MS appears to be increasing among women and diagnosis is occurring earlier, it becomes imperative to understand and optimize reproductive outcomes in this population. Our review provides reassurance that, in the majority of cases, women with MS can safely choose to become pregnant, give birth, and breastfeed children. Treatments and clinical interventions can be individualized for both the mother's MS and the reproductive course. The many unmet research needs identified in this review include the teratogenic risks (or safety) of most agents used to treat MS, better understanding of postpartum depression in mothers with MS, and the use and improvement of resources to support reproductive decision-making for women with MS.
AUTHOR INFORMATION
Harvard Medical School and the Departments of Neurology and Obstetrics and Gynecology, Brigham and Women's Hospital, Boston, Massachusetts; the Departments of Medical Genetics and Neurology, University of British Columbia, Vancouver, British Columbia, the Department of Pediatrics, Hospital for Sick Children, Toronto, Ontario, and the Department of Neurology, University of Alberta, Edmonton, Alberta, Canada; and St. Joseph Hospital Neurology Clinic, Ruhr University, Bochum, Germany.
Corresponding author: A. Dessa Sadovnick, PhD, S113-2211 Wesbrook Mall, Vancouver, BC V6T2B5, Canada; e-mail: [email protected].
The launch of MS-CERCH was funded by the Canadian Institutes of Health Research, Teva Neurosciences, and Biogen-Idec.
The authors thank members of MS-CERCH, who contributed comments to the sections specific to their area of expertise: Dr. V. Armenti (disease-specific registries), Dr. P. Duquette (neurology, pregnancy course after MS onset), Dr. A. Pupco (Motherisk, Teratology), Ms. C. Guimond (reproductive and genetic counseling for MS), and Ms. N. Razaz (children of MS parents).
Financial Disclosure The authors did not report any potential conflicts of interest.
REFERENCES
1. Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG. Multiple sclerosis. N Engl J Med 2000;343:938–52. Ovid Full Text Bibliographic Links
2. Bove R, Chitnis T. The role of gender and sex hormones in determining the onset and outcome of multiple sclerosis. Mult Scler 2014;20:520–6. Bibliographic Links
3. Sadovnick AD, Eisen K, Hashimoto SA, Farquhar R, Yee IM, Hooge J, et al.. Pregnancy and multiple sclerosis. A prospective study. Arch Neurol 1994;51:1120–4. Bibliographic Links
4. Rudick RA. Pregnancy and multiple sclerosis. Arch Neurol 1995;52:849–50. Ovid Full Text Bibliographic Links
5. Sweeney WJ. Pregnancy and multiple sclerosis. Am J Obstet Gynecol 1953;66:124–30. Bibliographic Links
6. Borisow N, Döring A, Pfueller CF, Paul F, Dörr J, Hellwig K. Expert recommendations to personalization of medical approaches in treatment of multiple sclerosis: an overview of family planning and pregnancy. EPMA J 2012;3:9. Bibliographic Links
7. McCombe PA, Greer JM. Female reproductive issues in multiple sclerosis. Mult Scler 2013;19:392–402. Bibliographic Links
8. Miller DH, Fazekas F, Montalban X, Reingold SC, Trojano M. Pregnancy, sex and hormonal factors in multiple sclerosis. Mult Scler 2014;20:527–36. Bibliographic Links
9. Bodiguel E, Bensa C, Brassat D, Laplaud D, Le Page E, Ouallet JC, et al.. Multiple sclerosis and pregnancy. Rev Neurol (Paris) 2014;170:247–65.
10. Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception 2011;84:478–85. Bibliographic Links
11. Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plann 2010;41:241–50. Bibliographic Links
12. Skinner S, Guimond C, Butler R, Dwosh E, Traboulsee AL, Sadovnick AD. An assessment of genetic counseling services for individuals with multiple sclerosis. J Genet Couns 2014 July 5 [Epub ahead of print].
13. Romano AM. A Changing Landscape: Implications of Pregnant Women's Internet Use for Childbirth Educators. J Perinat Educ 2007;16:18–24. Bibliographic Links
14. Lagan BM, Sinclair M, Kernohan WG. What is the impact of the Internet on decision-making in pregnancy? A global study. Birth 2011;38:336–45. Ovid Full Text Bibliographic Links
15. Birk K, Ford C, Smeltzer S, Ryan D, Miller R, Rudick RA. The clinical course of multiple sclerosis during pregnancy and the puerperium. Arch Neurol 1990;47:738–42. Bibliographic Links
16. Bernardi S, Grasso MG, Bertollini R, Orzi F, Fieschi C. The influence of pregnancy on relapses in multiple sclerosis: a cohort study. Acta Neurol Scand 1991;84:403–6. Bibliographic Links
17. Worthington J, Jones R, Crawford M, Forti A. Pregnancy and multiple sclerosis—a 3-year prospective study. J Neurol 1994;241:228–33. Bibliographic Links
18. Roullet E, Verdier-Taillefer MH, Amarenco P, Gharbi G, Alperovitch A, Marteau R. Pregnancy and multiple sclerosis: a longitudinal study of 125 remittent patients. J Neurol Neurosurg Psychiatry 1993;56:1062–5. Bibliographic Links
19. Salemi G, Callari G, Gammino M, Battaglieri F, Cammarata E, Cuccia G, et al.. The relapse rate of multiple sclerosis changes during pregnancy: a cohort study. Acta Neurol Scand 2004;110:23–6. Ovid Full Text Bibliographic Links
20. Fragoso YD, Finkelsztejn A, Comini-Frota ER, da Gama PD, Grzesiuk AK, Khouri JM, et al.. Pregnancy and multiple sclerosis: the initial results from a Brazilian database. Arq Neuropsiquiatr 2009;67:657–60. Bibliographic Links
21. Fernández Liguori N, Klajn D, Acion L, Cáceres F, Calle A, Carrá A, et al.. Epidemiological characteristics of pregnancy, delivery, and birth outcome in women with multiple sclerosis in Argentina (EMEMAR study). Mult Scler 2009;15:555–62. Bibliographic Links
22. Neuteboom RF, Janssens AC, Siepman TA, Hoppenbrouwers IA, Ketelslegers IA, Jafari N, et al.. Pregnancy in multiple sclerosis: clinical and self-report scales. J Neurol 2012;259:311–7. Ovid Full Text Bibliographic Links
23. Hellwig K, Brune N, Haghikia A, Müller T, Schimrigk S, Schwödiauer V, et al.. Reproductive counselling, treatment and course of pregnancy in 73 German MS patients. Acta Neurol Scand 2008;118:24–8. Ovid Full Text Bibliographic Links
24. Paavilainen T, Kurki T, Parkkola R, Färkkilä M, Salonen O, Dastidar P, et al.. Magnetic resonance imaging of the brain used to detect early post-partum activation of multiple sclerosis. Eur J Neurol 2007;14:1216–21. Ovid Full Text Bibliographic Links
25. Finkelsztejn A, Brooks JB, Paschoal FM Jr, Fragoso YD. What can we really tell women with multiple sclerosis regarding pregnancy? A systematic review and meta-analysis of the literature. BJOG 2011;118:790–7. Ovid Full Text Bibliographic Links
26. French J, Gronseth G. Lost in a jungle of evidence: we need a compass. Neurology 2008;71:1634–8. Ovid Full Text Bibliographic Links
27. D'hooghe MB, D'Hooghe T, De Keyser J. Female gender and reproductive factors affecting risk, relapses and progression in multiple sclerosis. Gynecol Obstet Invest 2013;75:73–84. Bibliographic Links
28. Vukusic S, Hutchinson M, Hours M, Moreau T, Cortinovis-Tourniaire P, Adeleine P, et al.. Pregnancy and multiple sclerosis (the PRIMS study): clinical predictors of post-partum relapse. Brain 2004;127:1353–60. Ovid Full Text Bibliographic Links
29. Portaccio E, Ghezzi A, Hakiki B, Sturchio A, Martinelli V, Moiola L, et al.. Postpartum relapses increase the risk of disability progression in multiple sclerosis: the role of disease modifying drugs. J Neurol Neurosurg Psychiatry 2014;85:845–50. Ovid Full Text Bibliographic Links
30. Paavilainen T, Kurki T, Färkkilä M, Salonen O, Parkkola R, Airas L. Lower brain diffusivity in postpartum period compared to late pregnancy: results from a prospective imaging study of multiple sclerosis patients. Neuroradiology 2012;54:823–8. Bibliographic Links
31. Airas L, Saraste M, Rinta S, Elovaara I, Huang YH, Wiendl H; Finnish Multiple Sclerosis and Pregnancy Study Group. Immunoregulatory factors in multiple sclerosis patients during and after pregnancy: relevance of natural killer cells. Clin Exp Immunol 2008;151:235–43. Ovid Full Text Bibliographic Links
32. Airas L, Nikula T, Huang YH, Lahesmaa R, Wiendl H. Postpartum-activation of multiple sclerosis is associated with down-regulation of tolerogenic HLA-G. J Neuroimmunol 2007;187:205–11. Bibliographic Links
33. Sicotte NL, Liva SM, Klutch R, Pfeiffer P, Bouvier S, Odesa S, et al.. Treatment of multiple sclerosis with the pregnancy hormone estriol. Ann Neurol 2002;52:421–8. Bibliographic Links
34. Hughes SE, Spelman T, Gray OM, Boz C, Trojano M, Lugaresi A, et al.. Predictors and dynamics of postpartum relapses in women with multiple sclerosis. Mult Scler 2014;20:739–46. Bibliographic Links
35. Weinshenker BG, Hader W, Carriere W, Baskerville J, Ebers GC. The influence of pregnancy on disability from multiple sclerosis: a population-based study in Middlesex County, Ontario. Neurology 1989;39:1438–40.
36. Koch M, Uyttenboogaart M, Heersema D, Steen C, De Keyser J. Parity and secondary progression in multiple sclerosis. J Neurol Neurosurg Psychiatry 2009;80:676–8. Ovid Full Text Bibliographic Links
37. Ramagopalan S, Yee I, Byrnes J, Guimond C, Ebers G, Sadovnick D. Term pregnancies and the clinical characteristics of multiple sclerosis: a population based study. J Neurol Neurosurg Psychiatry 2012;83:793–5. Ovid Full Text Bibliographic Links
38. Runmarker B, Andersen O. Pregnancy is associated with a lower risk of onset and a better prognosis in multiple sclerosis. Brain 1995;118:253–61. Bibliographic Links
39. D'hooghe MB, Haentjens P, Nagels G, D'Hooghe T, De Keyser J. Menarche, oral contraceptives, pregnancy and progression of disability in relapsing onset and progressive onset multiple sclerosis. J Neurol 2012;259:855–61. Ovid Full Text Bibliographic Links
40. Verdru P, Theys P, D'Hooghe MB, Carton H. Pregnancy and multiple sclerosis: the influence on long term disability. Clin Neurol Neurosurg 1994;96:38–41. Bibliographic Links
41. Keyhanian K, Davoudi V, Etemadifar M, Amin M. Better prognosis of multiple sclerosis in patients who experienced a full-term pregnancy. Eur Neurol 2012;68:150–5. Bibliographic Links
42. D'hooghe MB, Haentjens P, Nagels G, D'Hooghe T, De Keyser J. Menarche, oral contraceptives, pregnancy and progression of disability in relapsing onset and progressive onset multiple sclerosis. J Neurol 2012;259:855–61. Ovid Full Text Bibliographic Links
43. D'hooghe MB, Nagels G, Uitdehaag BM. Long-term effects of childbirth in MS. J Neurol Neurosurg Psychiatry 2010;81:38–41. Ovid Full Text Bibliographic Links
44. Karp I, Manganas A, Sylvestre MP, Ho A, Roger E, Duquette P. Does pregnancy alter the long-term course of multiple sclerosis? Ann Epidemiol 2014;24:504–8.e2.
45. Alwan S, Yee IM, Dybalski M, Guimond C, Dwosh E, Greenwood TM, et al.. Reproductive decision making after the diagnosis of multiple sclerosis (MS). Mult Scler 2013;19:351–8. Bibliographic Links
46. Demirkiran M, Sarica Y, Uguz S, Yerdelen D, Aslan K. Multiple sclerosis patients with and without sexual dysfunction: are there any differences? Mult Scler 2006;12:209–14.
47. Grinsted L, Heltberg A, Hagen C, Djursing H. Serum sex hormone and gonadotropin concentrations in premenopausal women with multiple sclerosis. J Intern Med 1989;226:241–4. Bibliographic Links
48. Lombardi G, Celso M, Bartelli M, Cilotti A, Del Popolo G. Female sexual dysfunction and hormonal status in multiple sclerosis patients. J Sex Med 2011;8:1138–46. Ovid Full Text Bibliographic Links
49. Sloka JS, Phillips PW, Stefanelli M, Joyce C. Co-occurrence of autoimmune thyroid disease in a multiple sclerosis cohort. J Autoimmune Dis 2005;2:9.
50. Marrie RA, Yu BN, Leung S, Elliott L, Warren S, Wolfson C, et al.. The incidence and prevalence of thyroid disease do not differ in the multiple sclerosis and general populations: a validation study using administrative data. Neuroepidemiology 2012;39:135–42. Bibliographic Links
51. Biogen Idec. Tysabri® (natalizumab). Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/125104s0576lbl.pdf. Retrieved October 18, 2014.
52. Biogen Idec. Avonex® (interferon [beta]-1a). Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2007/103628s5115lbl.pdf. Retrieved June 1, 2014.
53. Novartis Pharmaceuticals. Gilenya® (fingolimod). Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/022527s008lbl.pdf. Retrieved June 1, 2014.
54. Teva Pharmaceuticals. Copaxone® (glatiramer acetate). Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020622s057lbl.pdf. Retrieved June 1, 2014.
55. Alroughani R. Fingolimod-associated amenorrhea: a report of three cases. Mult Scler 2014 Feb 10 [Epub ahead of print].
56. Harward LE, Mitchell K, Pieper C, Copland S, Criscione-Schreiber LG, Clowse ME. The impact of cyclophosphamide on menstruation and pregnancy in women with rheumatologic disease. Lupus 2013;22:81–6. Bibliographic Links
57. Cocco E, Sardu C, Gallo P, Capra R, Amato MP, Trojano M, et al.. Frequency and risk factors of mitoxantrone-induced amenorrhea in multiple sclerosis: the FEMIMS study. Mult Scler 2008;14:1225–33. Bibliographic Links
58. Linssen WH, Notermans NC, Hommes OR, Rolland R. Amenorrhea after immunosuppressive treatment of multiple sclerosis. Acta Neurol Scand 1987;76:204–9. Bibliographic Links
59. Cavalla P, Rovei V, Masera S, Vercellino M, Massobrio M, Mutani R, et al.. Fertility in patients with multiple sclerosis: current knowledge and future perspectives. Neurol Sci 2006;27:231–9. Ovid Full Text Bibliographic Links
60. Jalkanen A, Alanen A, Airas L; Finnish Multiple Sclerosis and Pregnancy Study Group. Pregnancy outcome in women with multiple sclerosis: results from a prospective nationwide study in Finland. Mult Scler 2010;16:950–5. Bibliographic Links
61. Sutcliffe AG, Ludwig M. Outcome of assisted reproduction. Lancet 2007;370:351–9. Bibliographic Links
62. Hellwig K, Correale J. Artificial reproductive techniques in multiple sclerosis. Clin Immunol 2013;149:219–24. Bibliographic Links
63. Laplaud DA, Lefrère F, Leray E, Barrière P, Wiertlewski S. Increased risk of relapse in multiple sclerosis patients after ovarian stimulation for in vitro fertilization [in French]. Gynecol Obstet Fertil 2007;35:1047–50. Bibliographic Links
64. Hellwig K, Beste C, Brune N, Haghikia A, Müller T, Schimrigk S, et al.. Increased MS relapse rate during assisted reproduction technique. J Neurol 2008;255:592–3. Ovid Full Text Bibliographic Links
65. Hellwig K, Schimrigk S, Beste C, Muller T, Gold R. Increase in relapse rate during assisted reproduction technique in patients with multiple sclerosis. Eur Neurol 2009;61:65–8. Bibliographic Links
66. Michel L, Foucher Y, Vukusic S, Confavreux C, de Sèze J, Brassat D, et al.. Increased risk of multiple sclerosis relapse after in vitro fertilisation. J Neurol Neurosurg Psychiatry 2012;83:796–802. Ovid Full Text Bibliographic Links
67. Correale J, Farez MF, Ysrraelit MC. Increase in multiple sclerosis activity after assisted reproduction technology. Ann Neurol 2012;72:682–94. Ovid Full Text Bibliographic Links
68. Matthiesen SM, Frederiksen Y, Ingerslev HJ, Zachariae R. Stress, distress and outcome of assisted reproductive technology (ART): a meta-analysis. Hum Reprod 2011;26:2763–76. Ovid Full Text Bibliographic Links
69. Sena A, Couderc R, Vasconcelos JC, Ferret-Sena V, Pedrosa R. Oral contraceptive use and clinical outcomes in patients with multiple sclerosis. J Neurol Sci 2012;317:47–51. Bibliographic Links
70. Gava G, Bartolomei I, Costantino A, Berra M, Venturoli S, Salvi F, et al.. Long-term influence of combined oral contraceptive use on the clinical course of relapsing-remitting multiple sclerosis. Fertil Steril 2014;102:116–22. Bibliographic Links
71. Holmqvist P, Hammar M, Landtblom AM, Brynhildsen J. Age at onset of multiple sclerosis is correlated to use of combined oral contraceptives and childbirth before diagnosis. Fertil Steril 2010;94:2835–7. Bibliographic Links
72. Alonso A, Jick SS, Olek MJ, Ascherio A, Jick H, Hernán MA. Recent use of oral contraceptives and the risk of multiple sclerosis. Arch Neurol 2005;62:1362–5. Ovid Full Text Bibliographic Links
73. David OJ, Ocwieja M, Meiser K, Emotte C, Jakab A, Wemer J, et al.. Pharmacokinetics of fingolimod (FTY720) and a combined oral contraceptive coadministered in healthy women: drug–drug interaction study results. Int J Clin Pharmacol Ther 2012;50:540–4. Bibliographic Links
74. Clinical management guidelines for obstetrician-gynecologists. ACOG Practice Bulletin No. 81. American College of Obstetricians and Gynecologists. Obstet Gynecol 2007;109:1233–48.
75. Brown HL, Graves CR. Smoking and marijuana use in pregnancy. Clin Obstet Gynecol 2013;56:107–13. Ovid Full Text Bibliographic Links
76. Aghajafari F, Nagulesapillai T, Ronksley PE, Tough SC, O'Beirne M, Rabi DM. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: systematic review and meta-analysis of observational studies. BMJ 2013;346:f1169. Bibliographic Links
77. Christesen HT, Falkenberg T, Lamont RF, Jørgensen JS. The impact of vitamin D on pregnancy: a systematic review. Acta Obstet Gynecol Scand 2012;91:1357–67. Ovid Full Text Bibliographic Links
78. Tremlett H, van der Mei IA, Pittas F, Blizzard L, Paley G, Mesaros D, et al.. Monthly ambient sunlight, infections and relapse rates in multiple sclerosis. Neuroepidemiology 2008;31:271–9. Bibliographic Links
79. Mowry EM, Krupp LB, Milazzo M, Chabas D, Strober JB, Belman AL, et al.. Vitamin D status is associated with relapse rate in pediatric-onset multiple sclerosis. Ann Neurol 2010;67:618–24. Bibliographic Links
80. Mowry EM, Waubant E, McCulloch CE, Okuda DT, Evangelista AA, Lincoln RR, et al.. Vitamin D status predicts new brain magnetic resonance imaging activity in multiple sclerosis. Ann Neurol 2012;72:234–40. Ovid Full Text Bibliographic Links
81. Mowry EM. Vitamin D: evidence for its role as a prognostic factor in multiple sclerosis. J Neurol Sci 2011;311:19–22.
82. Dobson R, Giovannoni G, Ramagopalan S. The month of birth effect in multiple sclerosis: systematic review, meta-analysis and effect of latitude. J Neurol Neurosurg Psychiatry 2013;84:427–32. Ovid Full Text Bibliographic Links
83. Chaudhuri A. Why we should offer routine vitamin D supplementation in pregnancy and childhood to prevent multiple sclerosis. Med Hypotheses 2005;64:608–18. Bibliographic Links
84. Grytten N, Torkildsen Ø, Aarseth JH, Benjaminsen E, Celius EG, Dahl OP, et al.. Month of birth as a latitude-dependent risk factor for multiple sclerosis in Norway. Mult Scler 2013;19:1028–34. Bibliographic Links
85. Staples J, Ponsonby AL, Lim L. Low maternal exposure to ultraviolet radiation in pregnancy, month of birth, and risk of multiple sclerosis in offspring: longitudinal analysis. BMJ 2010;340:c1640. Ovid Full Text Bibliographic Links
86. Thorne-Lyman A, Fawzi WW. Vitamin D during pregnancy and maternal, neonatal and infant health outcomes: a systematic review and meta-analysis. Paediatr Perinat Epidemiol 2012;26(suppl 1):75–90. Bibliographic Links
87. Vitamin D: screening and supplementation during pregnancy. Committee Opinion No. 495. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:197–8.
88. International Multiple Sclerosis Genetics Consortium (IMSGC), Beecham AH, Patsopoulos NA, Xifara DK, Davis MF, Kemppinen A, Cotsapas C, et al.. Analysis of immune-related loci identifies 48 new susceptibility variants for multiple sclerosis. Nat Genet 2013;45:1353–60.
89. Langagergaard V, Pedersen L, Gislum M, Nørgard B, Sørensen HT. Birth outcome in women treated with azathioprine or mercaptopurine during pregnancy: a Danish nationwide cohort study. Aliment Pharmacol Ther 2007;25:73–81. Ovid Full Text Bibliographic Links
90. Sadovnick AD, Ebers GC. Genetics of multiple sclerosis. Neurol Clin 1995;13:99–118.
91. Ebers GC, Yee IM, Sadovnick AD, Duquette P. Conjugal multiple sclerosis: population-based prevalence and recurrence risks in offspring. Canadian Collaborative Study Group. Ann Neurol 2000;48:927–31. Bibliographic Links
92. Coyle PK, Christie S, Fodor P, Fuchs K, Giesser B, Gutierrez A, et al.. Multiple sclerosis gender issues: clinical practices of women neurologists. Mult Scler 2004;10:582–8. Bibliographic Links
93. Lu E, Wang BW, Guimond C, Synnes A, Sadovnick D, Tremlett H. Disease-modifying drugs for multiple sclerosis in pregnancy: a systematic review. Neurology 2012;79:1130–5. Ovid Full Text Bibliographic Links
94. Wundes A, Pebdani RN, Amtmann D. What do healthcare providers advise women with multiple sclerosis regarding pregnancy? Mult Scler Int 2014;2014:819216.
95. Wehman-Tubbs K, Yale SH, Rolak LA. Insight into multiple sclerosis. Clin Med Res 2005;3:41–4. Bibliographic Links
96. Castillo-Trivino T, Braithwaite D, Bacchetti P, Waubant E. Rituximab in relapsing and progressive forms of multiple sclerosis: a systematic review. PLoS One 2013;8:e66308. Bibliographic Links
97. Berger JR, Centonze D, Comi G, Confavreux C, Cutter G, Giovannoni G, et al.. Considerations on discontinuing natalizumab for the treatment of multiple sclerosis. Ann Neurol 2010;68:409–11. Bibliographic Links
98. Martinelli V, Colombo B, Dalla Costa G, Dalla Libera D, Moiola L, Falini A, et al.. Recurrent disease-activity rebound in a patient with multiple sclerosis after natalizumab discontinuations for pregnancy planning. Mult Scler 2013 Jun 17 [Epub ahead of print].
99. Sempere AP, Berenguer-Ruiz L, Feliu-Rey E. Rebound of disease activity during pregnancy after withdrawal of fingolimod. Eur J Neurol 2013;20:e109–10. Ovid Full Text Bibliographic Links
100. Achiron A, Kishner I, Dolev M, Stern Y, Dulitzky M, Schiff E, et al.. Effect of intravenous immunoglobulin treatment on pregnancy and postpartum-related relapses in multiple sclerosis. J Neurol 2004;251:1133–7. Ovid Full Text Bibliographic Links
101. Haas J, Hommes OR. A dose comparison study of IVIG in postpartum relapsing-remitting multiple sclerosis. Mult Scler 2007;13:900–8. Bibliographic Links
102. Hellwig K, Beste C, Schimrigk S, Chan A. Immunomodulation and postpartum relapses in patients with multiple sclerosis. Ther Adv Neurol Disord 2009;2:7–11. Bibliographic Links
103. Ferrero S, Esposito F, Pretta S, Ragni N. Fetal risks related to the treatment of multiple sclerosis during pregnancy and breastfeeding. Expert Rev Neurother 2006;6:1823–31. Ovid Full Text Bibliographic Links
104. Park-Wyllie L, Mazzotta P, Pastuszak A, Moretti ME, Beique L, Hunnisett L, et al.. Birth defects after maternal exposure to corticosteroids: prospective cohort study and meta-analysis of epidemiological studies. Teratology 2000;62:385–92. Bibliographic Links
105. Pradat P, Robert-Gnansia E, Di Tanna GL, Rosano A, Lisi A, Mastroiacovo P; Contributors to the MADRE database. First trimester exposure to corticosteroids and oral clefts. Birth Defects Res A Clin Mol Teratol 2003;67:968–70. Bibliographic Links
106. Rodríguez-Pinilla E, Martinez-Frías ML. Corticosteroids during pregnancy and oral clefts: a case-control study. Teratology 1998;58:2–5. Bibliographic Links
107. Carmichael SL, Shaw GM. Maternal corticosteroid use and risk of selected congenital anomalies. Am J Med Genet 1999;86:242–4. Bibliographic Links
108. Hviid A, Mølgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacial clefts. CMAJ 2011;183:796–804. Ovid Full Text Bibliographic Links
109. Hoes JN, Jacobs JW, Boers M, Boumpas D, Buttgereit F, Caeyers N, et al.. EULAR evidence-based recommendations on the management of systemic glucocorticoid therapy in rheumatic diseases. Ann Rheum Dis 2007;66:1560–7. Ovid Full Text Bibliographic Links
110. Namazy JA, Murphy VE, Powell H, Gibson PG, Chambers C, Schatz M. Effects of asthma severity, exacerbations and oral corticosteroids on perinatal outcomes. Eur Respir J 2013;41:1082–90. Bibliographic Links
111. Elliott AB, Chakravarty EF. Immunosuppressive medications during pregnancy and lactation in women with autoimmune diseases. Womens Health (Lond Engl) 2010;6:431–40.
112. Webb JA, Thomsen HS, Morcos SK; Members of Contrast Media Safety Committee of European Society of Urogenital Radiology (ESUR). The use of iodinated and gadolinium contrast media during pregnancy and lactation. Eur Radiol 2005;15:1234–40.
113. American College of Radiology. ACR guidelines and technical standards. Practice guideline for imaging pregnant or potentially pregnant adolescents and women with ionizing radiation. Reston (VA): American College of Radiology; 2008.
114. Kanal E, Shellock FG, Talagala L. Safety considerations in MR imaging. Radiology 1990;176:593–606. Bibliographic Links
115. Guidelines for diagnostic imaging during pregnancy. ACOG Committee Opinion No. 299. American College of Obstetricians and Gynecologists. Obstet Gynecol 2004;104:647–51.
116. ACR Committee on Drugs and Contrast Media. Administration of contrast media to breast-feeding mothers. In: ACR manual on contrast media, Version 9. Reston (VA): American College of Radiology; 2013.p. 97–8.
117. American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics 2001;108:776–89. Ovid Full Text Bibliographic Links
118. Kelly VM, Nelson LM, Chakravarty EF. Obstetric outcomes in women with multiple sclerosis and epilepsy. Neurology 2009;73:1831–6. Ovid Full Text Bibliographic Links
119. Lu E, Zhu F, van der Kop M, Dahlgren L, Synnes A, Sadovnick A, et al.. Labor induction and augmentation in women with multiple sclerosis. Mult Scler 2013;19:1182–9.
120. Lu E, Zhao Y, Zhu F, van der Kop ML, Synnes A, Dahlgren L, et al.. Birth hospitalization in mothers with multiple sclerosis and their newborns. Neurology 2013;80:447–52. Ovid Full Text Bibliographic Links
121. Dahl J, Myhr KM, Daltveit AK, Hoff JM, Gilhus NE. Pregnancy, delivery, and birth outcome in women with multiple sclerosis. Neurology 2005;65:1961–3. Ovid Full Text Bibliographic Links
122. Dahl J, Myhr KM, Daltveit AK, Gilhus NE. Planned vaginal births in women with multiple sclerosis: delivery and birth outcome. Acta Neurol Scand Suppl 2006;183:51–4. Bibliographic Links
123. Chen YH, Lin HL, Lin HC. Does multiple sclerosis increase risk of adverse pregnancy outcomes? A population-based study. Mult Scler 2009;15:606–12. Bibliographic Links
124. Mueller BA, Zhang J, Critchlow CW. Birth outcomes and need for hospitalization after delivery among women with multiple sclerosis. Am J Obstet Gynecol 2002;186:446–52. Ovid Full Text Bibliographic Links
125. van der Kop ML, Pearce MS, Dahlgren L, Synnes A, Sadovnick D, Sayao AL, et al.. Neonatal and delivery outcomes in women with multiple sclerosis. Ann Neurol 2011;70:41–50. Ovid Full Text Bibliographic Links
126. Lu E, Zhao Y, Dahlgren L, Preston R, van der Kop M, Synnes A, et al.. Obstetrical epidural and spinal anesthesia in multiple sclerosis. J Neurol 2013;260:2620–8. Bibliographic Links
127. Dahl J, Myhr KM, Daltveit AK, Gilhus NE. Pregnancy, delivery and birth outcome in different stages of maternal multiple sclerosis. J Neurol 2008;255:623–7. Ovid Full Text Bibliographic Links
128. Dalmas AF, Texier C, Ducloy-Bouthors AS, Krivosic-Horber R. Obstetrical analgesia and anaesthesia in multiple sclerosis [in French]. Ann Fr Anesth Reanim 2003;22:861–4. Bibliographic Links
129. Martucci G, Di Lorenzo A, Polito F, Acampa L. A 12-month follow-up for neurological complication after subarachnoid anesthesia in a parturient affected by multiple sclerosis. Eur Rev Med Pharmacol Sci 2011;15:458–60. Bibliographic Links
130. Drake E, Drake M, Bird J, Russell R. Obstetric regional blocks for women with multiple sclerosis: a survey of UK experience. Int J Obstet Anesth 2006;15:115–23. Bibliographic Links
131. Vukusic S, Confavreux C. Multiple sclerosis and pregnancy [in French]. Rev Neurol (Paris) 2006;162:299–309.
132. Pasto L, Portaccio E, Ghezzi A, Hakiki B, Giannini M, Razzolini L, et al.. Epidural analgesia and cesarean delivery in multiple sclerosis post-partum relapses: the Italian cohort study. BMC Neurol 2012;12:165. Bibliographic Links
133. Bader AM, Hunt CO, Datta S, Naulty JS, Ostheimer GW. Anesthesia for the obstetric patient with multiple sclerosis. J Clin Anesth 1988;1:21–4. Bibliographic Links
134. Finucane BT, Terblanche OC. Prolonged duration of anesthesia in a patient with multiple sclerosis following paravertebral block. Can J Anaesth 2005;52:493–7. Bibliographic Links
135. Rabadán Diaz JV, López Moreno JA, Soria Quiles A, Del Pino Moreno AL. Neurological deficit during recovery from cesarean section under spinal anesthesia after the appearance of undiagnosed multiple sclerosis [in Spanish]. Rev Esp Anestesiol Reanim 2006;53:673–4. Bibliographic Links
136. Orvieto R, Achiron R, Rotstein Z, Noy S, Bar-Hava I, Achiron A. Pregnancy and multiple sclerosis: a 2-year experience. Eur J Obstet Gynecol Reprod Biol 1999;82:191–4. Bibliographic Links
137. Poser S, Poser W. Multiple sclerosis and gestation. Neurology 1983;33:1422–7. Ovid Full Text Bibliographic Links
138. Finkelsztejn A, Fragoso YD, Ferreira ML, Lana-Peixoto MA, Alves-Leon SV, Gomes S, et al.. The Brazilian database on pregnancy in multiple sclerosis. Clin Neurol Neurosurg 2011;113:277–80. Bibliographic Links
139. World Health Organization. Pregnancy, childbirth, postpartum and newborn care—a guide for essential practice. 2006 ed. Geneva (Switzerland): World Health Organization, Department of Making Pregnancy Safer; 2006.
140. Pakpoor J, Disanto G, Lacey MV, Hellwig K, Giovannoni G, Ramagopalan SV. Breastfeeding and multiple sclerosis relapses: a meta-analysis. J Neurol 2012;259:2246–8. Bibliographic Links
141. Gulick EE. Influence of infant feeding method on postpartum relapse of mothers with MS. Int J MS Care 2002;4:4–14.
142. Langer-Gould A, Huang SM, Gupta R, Leimpeter AD, Greenwood E, Albers KB, et al.. Exclusive breastfeeding and the risk of postpartum relapses in women with multiple sclerosis. Arch Neurol 2009;66:958–63. Ovid Full Text Bibliographic Links
143. Hellwig K, Haghikia A, Rockhoff M, Gold R. Multiple sclerosis and pregnancy: experience from a nationwide database in Germany. Ther Adv Neurol Disord 2012;5:247–53. Bibliographic Links
144. Nelson LM, Franklin GM, Jones MC. Risk of multiple sclerosis exacerbation during pregnancy and breast-feeding. JAMA 1988;259:3441–3. Bibliographic Links
145. Confavreux C, Hutchinson M, Hours MM, Cortinovis-Tourniaire P, Moreau T. Rate of pregnancy-related relapse in multiple sclerosis. Pregnancy in Multiple Sclerosis Group. N Engl J Med 1998;339:285–91. Ovid Full Text Bibliographic Links
146. Portaccio E, Ghezzi A, Hakiki B, Martinelli V, Moiola L, Patti F, et al.. Breastfeeding is not related to postpartum relapses in multiple sclerosis. Neurology 2011;77:145–50. Ovid Full Text Bibliographic Links
147. Hollis BW, Wagner CL. Assessment of dietary vitamin D requirements during pregnancy and lactation. Am J Clin Nutr 2004;79:717–26. Bibliographic Links
148. Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266–81. Ovid Full Text Bibliographic Links
149. Langer-Gould A, Huang S, Van Den Eeden SK, Gupta R, Leimpeter AD, Albers KB, et al.. Vitamin D, pregnancy, breastfeeding, and postpartum multiple sclerosis relapses. Arch Neurol 2011;68:310–3. Ovid Full Text Bibliographic Links
150. National Institutes of Health. LactMed. Available at: http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT. Retrieved June 1, 2014.
151. Hale TW. Medications and mothers' milk. 15th ed. Amarillo (TX): Hale Publishing; 2012.
152. Koren G. Medication safety in pregnancy and breastfeeding. New York (NY): McGraw-Hill; 2007.
153. Hellwig K, Gold R. Glatiramer acetate and interferon-beta throughout gestation and postpartum in women with multiple sclerosis. J Neurol 2011;258:502–3. Ovid Full Text Bibliographic Links
154. Hale TW, Siddiqui AA, Baker TE. Transfer of interferon [beta]-1a into human breastmilk. Breastfeed Med 2012;7:123–5. Bibliographic Links
155. Houtchens MK, Kolb CM. Multiple sclerosis and pregnancy: therapeutic considerations. J Neurol 2013;260:1202–14. Bibliographic Links
156. de Seze J, Chapelotte M, Delalande S, Ferriby D, Stojkovic T, Vermersch P. Intravenous corticosteroids in the postpartum period for reduction of acute exacerbations in multiple sclerosis. Mult Scler 2004;10:596–7. Bibliographic Links
157. Greenberger PA, Odeh YK, Frederiksen MC, Atkinson AJ Jr. Pharmacokinetics of prednisolone transfer to breast milk. Clin Pharmacol Ther 1993;53:324–8. Bibliographic Links
158. Ost L, Wettrell G, Björkhem I, Rane A. Prednisolone excretion in human milk. J Pediatr 1985;106:1008–11. Bibliographic Links
159. McKenzie SA, Selley JA, Agnew JE. Secretion of prednisolone into breast milk. Arch Dis Child 1975;50:894–6. Bibliographic Links
160. Haas J. High dose IVIG in the post partum period for prevention of exacerbations in MS. Mult Scler 2000;6(suppl 2):S18–20. Bibliographic Links
161. Jalkanen A, Saraste M, Gfeller A, Surcel HM, Airas L. Increased thyroid autoimmunity among women with multiple sclerosis in the postpartum setting. Mult Scler 2013;19:1734–42. Bibliographic Links
162. O'Hara MW, McCabe JE. Postpartum depression: current status and future directions. Annu Rev Clin Psychol 2013;9:379–407. Bibliographic Links
163. Feinstein A. Multiple sclerosis and depression. Mult Scler 2011;17:1276–81. Bibliographic Links
164. Arnett PA, Barwick FH, Beeney JE. Depression in multiple sclerosis: review and theoretical proposal. J Int Neuropsychol Soc 2008;14:691–724. Bibliographic Links
165. Gulick EE, Kim S. Postpartum emotional distress in mothers with multiple sclerosis. J Obstet Gynecol Neonatal Nurs 2004;33:729–38. Ovid Full Text Bibliographic Links
166. Gulick EE. Adaptation of the postpartum support questionnaire for mothers with multiple sclerosis. Res Nurs Health 2003;26:30–9.
167. Gulick EE. Postpartum functioning in mothers with multiple sclerosis. West J Nurs Res 2007;29:589–602. Ovid Full Text Bibliographic Links
168. Ross LE, Grigoriadis S, Mamisashvili L, Vonderporten EH, Roerecke M, Rehm J, et al.. Selected pregnancy and delivery outcomes after exposure to antidepressant medication: a systematic review and meta-analysis. JAMA Psychiatry 2013;70:436–43.
169. Gibson J, McKenzie-McHarg K, Shakespeare J, Price J, Gray R. A systematic review of studies validating the Edinburgh Postnatal Depression Scale in antepartum and postpartum women. Acta Psychiatr Scand 2009;119:350–64. Ovid Full Text Bibliographic Links
170. Sanofi Aventis. Aubagio® (teriflunomide). Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/202992s000lbl.pdf. Retrieved June 1, 2014.