Vaccinations in multiple sclerosis patients receiving disease-modifying drugs
Why is this review important?
Recent advances in therapies have provided individuals with multiple sclerosis (MS) with a wide range of options for the management of their disease. These options include disease-modifying drugs (DMDs), which enable health care providers to better tailor MS treatments to each individual’s needs.
However, many DMDs for MS work by suppressing or modifying the immune system, which can decrease the body’s ability to fight infection effectively. Immunosuppressive medications can make people more susceptible to new infections and may also reactivate or worsen existing infections. This vulnerability has become even more concerning because of the recent spread of the infection caused by a novel coronavirus (SARS-CoV-2) around the world.
Experts in the management of MS across the globe are recommending preventive strategies, including vaccination against certain communicable diseases, to minimize the adverse effects of DMDs and allow people to experience the benefits of these therapies. In the context of the ongoing coronavirus disease 2019 (COVID-19) pandemic, it is important to know whether vaccines are safe for individuals with MS, who should receive them, and when vaccination is recommended for optimal antibody response.
Which vaccines are safe for individuals with MS?
Vaccines work in different ways to trigger an immune response, which causes the human body to produce antibodies and white blood cells that can block a virus from infecting other cells. Some use an inactivated or weaker version of the virus, whereas others rely on the genetic code of a protein that causes the disease to cause this immune response.
Inactivated vaccines are recommended in all people with MS who have advanced disease or are being treated with immunosuppressive therapies. These include the influenza (flu) shot, which should be administered annually, as well as vaccines against tetanus, diphtheria, pneumococcal disease, and human papillomavirus. Shots to prevent hepatitis A and B viral infections are also recommended in high-risk individuals with MS. Substantial evidence published over the past two decades has shown that such vaccines do not increase the risk of MS onset or MS relapses.
Live (attenuated) vaccines, such as those against measles or varicella, cause a mild infection, which is not harmful in people with normal immune function. However, they are contraindicated for people treated with immunosuppressive therapies. Individuals with MS should complete live-vaccine immunizations 4 weeks before beginning DMD therapy.
Since 2020, several vaccines against SARS-CoV-2 have been developed around the world. Inactivated or RNA-based COVID-19 vaccines are currently recommended for all individuals with MS, especially those treated with DMDs. Immunosuppressed individuals should avoid the live attenuated versions of the COVID-19 shot.
When should vaccines be administered?
People with MS should receive the recommended vaccines as soon as they become available. In general, all vaccinations should be completed at least 2 weeks before beginning immunosuppressive therapy, however, health care providers can make recommendations on a case-by-case basis. Early administration of the vaccines increases an individual’s chance of having a good immune response and may also avoid potential interaction with immunosuppressive therapies.
People who receive immunosuppressive medications, and particularly those treated with antibodies that target a protein found on the surface of B cells (B cell-depleting therapies), may have a diminished response after receiving vaccines such as those against COVID-19 disease. These individuals should continue to follow personal protective measures against COVID-19, especially since there is limited information about the effectiveness of COVID-19 vaccines in people with a weakened immune system.
If you are diagnosed with MS, ask your health care provider about any vaccinations that are recommended, especially if you are prescribed immunosuppressive medications. Your health care provider will request a detailed medical history, including previous vaccinations and your history of infectious diseases, to determine whether you will need any vaccines before starting treatment with DMDs. Finding the best vaccination strategy for your case will eliminate unnecessary treatment delays and will reduce your risk of infection during immunosuppressive therapy.
Original Article
Vaccinations in multiple sclerosis patients receiving disease-modifying drugs
Current Opinion in Neurology
Otero-Romero, Susanaa,b; Ascherio, Albertoc,d; Lebrun-Frénay, Christinee
Abstract
Purpose of review
This review focuses on new evidence supporting the global immunization strategy for multiple sclerosis (MS) patients receiving disease-modifying drugs (DMDs), including the recently available vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
Recent findings
New data strengthen the evidence against a causal link between MS and vaccination. Recent consensus statements agree on the need to start vaccination early. Timings for vaccine administration should be adjusted to ensure safety and optimize vaccine responses, given the potential interference of DMDs. Patients treated with Ocrelizumab (and potentially other B-cell depleting therapies) are at risk of diminished immunogenicity to vaccines. This has relevant implications for the upcoming vaccination against SARS-CoV-2.
Summary
An early assessment and immunization of MS patients allows optimizing vaccine responses and avoiding potential interference with treatment plans. Vaccinations are safe and effective but some specific considerations should be followed when vaccinating before, during, and after receiving immunotherapy. A time-window for vaccination taking into account the kinetics of B cell repopulation could potentially improve vaccine responses. Further understanding of SARS-CoV-2 vaccine response dynamics in MS patients under specific therapies will be key for defining the best vaccination strategy.
INTRODUCTION
Over the last years, the long-term prognosis of multiple sclerosis (MS) has improved, largely due to the expanded use of a range of highly active disease-modifying drugs (DMDs) that have brought us closer to achieving a personalized treatment paradigm [1]. These DMDs include injectables (IFNbeta and glatiramer acetate), monoclonal antibodies (natalizumab, alemtuzumab, ocrelizumab, and ofatumumab), and oral agents (fingolimod, dimethyl fumarate, cladribine, teriflunomide, and ozanimod). Due to the drugs mechanisms of action, including alteration of lymphocyte trafficking, lymphocyte depletion, and disruption of lymphocyte replication, patients may be at risk of reactivating latent pathogens, worsening of asymptomatic chronic infections, and contracting de novo infections [2].
Individualized therapy must balance considerations around efficacy and side effects. There is now a consensus that it should also incorporate a set of preventive strategies into the disease management to minimize risk of infection [3,4], including vaccination. This has been a topic of growing interest over the past two years. Several guidelines and review documents have been produced, following previous experience with other auto-immune disorders [5].
This review will focus on the recently published evidence supporting the global immunization strategy for MS patients receiving DMDs, in terms of safety and timing for optimizing vaccine response. We will also discuss the implications of the newly available vaccines against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and their potential use in MS patients, in the context of the ongoing pandemic.
TEXT OF REVIEW
Safe use of vaccines in the multiple sclerosis population
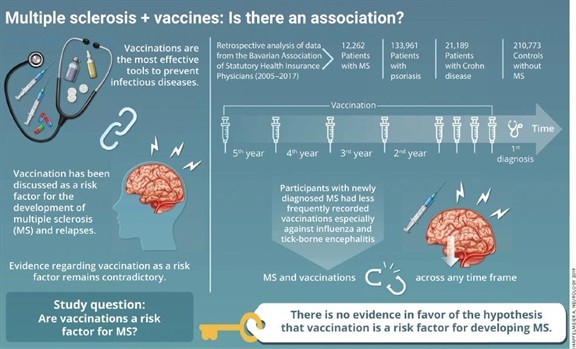
Historical concerns about the potential link between vaccination and the onset of MS have resulted in mistrust and very poor vaccination coverage of these patients. However, these studies were often underpowered and lacked adequate designs needed to confirm an association [6]. Substantial evidence published over the past two decades supports the absence of a causal link between inactivated vaccines such as influenza, tetanus, hepatitis B virus (HBV), and human papillomavirus (HPV) and the risk of MS onset or MS relapses [7,8]. This has been recently confirmed in a large case-control study using claims data from a population of 12,262 MS patients and 210,773 controls involving patients newly diagnosed with Crohn disease, psoriasis, and patients with no history of these autoimmune diseases. The absence of case ascertainment using chart review could introduce a potential bias, but the demonstration of decreasing odds with stricter criteria for case definition supports the robustness of the results [9▪▪].
Two additional studies focusing on the influenza and tick-borne encephalitis (TBE) vaccine show consistent findings. The safety of a seasonal influenza vaccine was evaluated in a cohort involving 108 MS patients treated with DMDs. There was no difference in relapse rates before and after vaccination. Only mild or moderate local or systemic reactions associated with the preceding vaccination were reported [10]. TBE vaccination showed good tolerability and safety profile for at least 6 months in 20 patients with MS on DMDs. MS disease activity was not increased after vaccination and disability remained stable during the year after vaccination. The noncontrolled nature of the design with a small sample size, and the lack of correlation between clinical and Magnetic Resonance Imaging disease activity are limitations of this study that warrants further confirmation [11▪].
The question on whether attenuated live vaccines and specifically yellow fever (YF) vaccine can be safely administered to MS patients remains a knowledge gap in need of further research. The only available studies are two small case series, which have important methodological limitations [12]. One [13], including seven MS patients, pointed toward an increased risk of relapses, whereas in the other [14▪], including 23 MS patients, YF vaccination was not associated with an increase in MS relapses or new or gadolinium-enhancing brain and/or spinal lesions. These null findings, if confirmed in larger populations, open the door for a potential change in the current need for caution.
Global vaccination approach and timing of vaccination
The substantial number of reviews and consensus statements [15–21] made available over the last two years covering aspects of immunization in MS patients generally agree on the overall vaccination strategy. An initial assessment including a detailed infectious disease history and a review of previous immunity to vaccine-preventable infections is highly recommended. This assessment should ideally be performed at the time of MS diagnosis, and as soon as possible in patients that are already receiving an immune MS therapy. This anticipation allows minimizing the risks associated with treatment delays caused by the need to complete vaccination schedules, as well as treatment withdrawals due to infectious complications. When indicated, vaccination should be offered to MS patients as soon as possible to optimize vaccine response and to avoid potential interference with treatment plans [15,17,18,20].
Live (or attenuated) vaccines, such as measles or varicella, are made up of live microorganisms that have attenuated virulence but stimulate the immune response, both cellular and humoral, in a similar way to natural infection, providing long-lasting protection. In patients already receiving an immunosuppressive treatment, attenuated vaccines are contraindicated due to the potential risk of vaccine-transmitted disease. Patients should complete live-vaccines immunizations schedules 4 weeks prior to onset of immunosuppressive therapy, including high doses of methylprednisolone (6 weeks according to the summary of product characteristics for Ocrelizumab and Alemtuzumab). Susceptible immunosuppressed patients can be offered a postexposure prophylaxis in the event of a risk exposure [22]. These patients can be considered for future immunization if immunosuppressive medication is interrupted for a period of time long enough so as to ensure clearance of the immunosuppressor. There are no specific indicators that guarantee immune restoration, but some authors suggest the usefulness of basic immunological parameters (such as subpopulations of CD4, CD8, and CD19 cells), as well as total immunoglobulin count [23].
Inactivated vaccines based on the whole microorganism or any of its fractions (polysaccharides, proteins, toxoids, subunits, etc.) do not have the ability to replicate in the host and thus can be used safely in MS patients, even in the presence of immunosuppressive therapy [24]. However, DMDs may modulate the effectiveness of these vaccines by lowering the capability of the immune system to mount an effective response. In this regard, a limited number of studies for some of the DMD in controlled settings, mainly focusing on the influenza vaccine, have shown reduced rates of seroprotection in patients treated with fingolimod [25] and teriflunomide [26,27], with a minor interference in those treated with natalizumab [28,29] and dimethyl fumarate [30]. The immune response does not seem to be altered according to a larger number of studies in patients receiving interferon-beta as compared to healthy controls or untreated MS patients [31]. These preserved responses to influenza vaccine have been recently confirmed in a real-life setting study. This supports the idea that seasonal influenza vaccination should be attempted in MS patients, even those under DMDs to achieve the best possible reductions in vaccination-preventable morbidity, hospitalization, and mortality [32].
B-cell depleting therapies are of major concern due to their direct impact on humoral responses. Decreased responses after Ocrelizumab therapy are shown in the VELOCE trial [33▪▪]. The frequency of seroconversion and the antibody titer was markedly reduced after 23-valent pneumococcal polysaccharide vaccine (23-PPV). Consistently, 23-PPV vaccine boosted by the 13-valent conjugate pneumococcal vaccine (13-PCV) 4 weeks after, did not markedly enhance the response to 12 serotypes, in common with 23-PPV. Additionally, the percentage of people with MS with a positive response to the antitetanus toxoid (TT)-containing vaccine were reduced in patients treated with ocrelizumab. However, the TT-specific antibody titers were generally above protective levels. This blunted vaccine response is expected also with the other anti-CD20 antibodies. An inefficient antibody response is reported in patients with other autoimmune diseases such as neuromyelitis optical spectrum disorders treated with Rituximab [34]. A single study evaluating patients receiving TT-containing vaccination, Haemophilus influenza type b conjugate vaccine and 23-PPV within six months of an Alemtuzumab infusion also resulted in a smaller proportion of responders as compared to healthy controls [35].
The optimal timing for vaccination should balance the urge for a fast protection and the probability of adequate vaccine response. In this regard, vaccines should be given at least 2 weeks before starting immunosuppressive therapies in those treatment-naïve patients, or in patients that have only been exposed to first-line immunomodulators [15,17,18,20]. Choosing the best time for immunization in patients who are already receiving an immunosuppressive drug, and specifically those under B-cell depleting therapy, is challenging as the impaired response will be maintained and/or increased following repeated infusions with increasing IgG hypogammaglobulinaemia [36]. However, despite a relative lack of memory B cells, CD19-repopulated individuals could mount a robust recall response [37]. In this context, some authors suggest the possibility of a time-window for vaccination due to the differential kinetics of B cells repopulation [38]. This could potentially be feasible with rituximab for which repletion occurs within approximately 6 months of treatment and is completed within 12 months due to repopulation of the immature/mature (naive) B cell pool. Timing required for this to occur for ocrelizumab is likely to be substantially longer (up to 18 months). The repopulation time for Cladribine and Alemtuzumab will be shorter with recovery of CD19 naive B cells within a median of 30 weeks and 6 months, respectively [39,40]. Such levels would require monitoring, as there is marked variability in repopulation kinetics between individuals. It would be a potential future strategy to optimize vaccine response that will need to be tested in properly designed observational studies.
Recommended vaccines
MS patients will require a general evaluation and updating of routine vaccines following local immunization schedules in each country. Some vaccines, such as seasonal influenza and PCVs, with extensive use in chronic conditions and immunosuppressed patients will also be specially recommended. Additionally, other specific vaccines with more restricted indications will be considered depending on the characteristics of the patient in terms of their risk-behaviors and past infections, as well as their DMD-specific potential risk of infection (see Table 1) [41▪]. There are not clear recommendations in this regard and the consensus documents refer to national guidelines on vaccination in immunocompromised patients. Of course, availability of vaccines and coverage by health-insurance in each country is determinant for the use of these vaccines with extended indication. Vaccination against the HBV, largely available in childhood immunization programs in many countries, could also be considered in young MS patients with negative Hepatitis B surface antibody (anti-HBs) who are at high risk of exposure. The HBV vaccine could be specially recommended for those patients who are candidates for anti-CD20 therapy for which severe occurrences or recurrences of hepatitis B infection have been described [42]. The recently approved herpes zoster inactivated recombinant vaccine is recommended for adults aged 50 years and older with a history of natural varicella infection. It would be specially recommended for those therapies with known increased risk of herpes-zoster infections such as fingolimod, natalizumab, cladribine, and alemtuzumab [41▪]. Finally, vaccination against HPV should be particularly considered for patients with upcoming fingolimod or alemtuzumab, as postmarket surveillance showed increased reports of warts and cervical dysplasia due to these two MS therapies [43].
New challenges ahead: vaccination against the severe acute respiratory syndrome coronavirus 2 infection
The coronavirus disease 2019 (COVID-19) pandemic caused by SARS-CoV-2 is posing a serious threat to public health worldwide [44]. Vaccination against SARS-CoV-2 might represent the most promising approach to halt the current COVID-19 pandemic. Several vaccine candidates are being developed at an unprecedented speed with a fast start and many steps executed in parallel [45]. Multiple platforms are currently under development including inactivated vaccines, nucleic acid vaccines, adenovirus-based vector vaccines, and recombinant subunit vaccines. Among those with the greatest potential for speed are the RNA-based platforms. RNA and DNA vaccines have the advantage of rapid production using synthetic processes that require no culture or fermentation [46].
Two different RNA-based vaccines (BNT162b2 developed by Pfizer-BioNTech and mRNA-1273 developed by Moderna) have been recently approved by the United States Food and Drug Administration (FDA) [47] and the European Medicines Agency (EMA) [48]. Results of the placebo-controlled phase III trials of these two RNA-based vaccine have shown promising results with a positive safety profile. The BNT162b2 vaccine trial involving 43,448 subjects reported a 95% efficacy in preventing Covid-19 after two doses. Similar vaccine efficacy was observed across subgroups defined by age, sex, race, ethnicity, baseline body-mass index, and the presence of coexisting conditions [49▪▪]. The mRNA-1273 vaccine was tested in 30,420 volunteers with a global efficacy of 94.1% in preventing symptomatic, laboratory-confirmed COVID-19 among persons without evidence of previous SARS-CoV-2 infection. Efficacy was similar for participants aged 65 or older. High efficacy (≥86%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions [50▪▪].The Oxford–AstraZeneca chimpanzee adenovirus vectored vaccine (AZD1222) has also been approved by EMA. The first reported results from two of the four ongoing controlled phase III trials have yielded conflicting results, with higher efficacy in the regimen with a lower initial dose (90%) as compared to the regimen of two standard doses (62%). This effect will need further exploration [51,52▪].
Available COVID trials have focused on efficacy outcomes in terms of prevention against symptomatic, laboratory-confirmed infection and prevention against severe disease and mortality. The latter are key secondary endpoints given that hospital and critical care admissions place the greatest burden on health-care systems [53]. A lingering question is whether the vaccine is capable of fighting asymptomatic infections. This would reduce the transmissibility of SARS-CoV-2 infection and would be key to shaping the course of the pandemic. Some of the ongoing studies, such as those on the AZD1222 vaccine, are monitoring participants for asymptomatic infections by collecting weekly swabs and will be able to provide some insight on this issue [51].
With vaccines against SARS-CoV-2 already available and starting to be deployed in different countries, questions on their use in the MS population are on the spotlight. Specific data to establish vaccine safety and efficacy in the MS population are currently not available and ongoing collaborative efforts and data-sharing initiatives will be of utmost importance in the following months [54]. The Center of Disease Control and Prevention (CDC) has issued specific recommendations that include patients with autoimmune conditions. Despite limited numbers, no imbalances were observed in the occurrence of symptoms consistent with inflammatory disorders in the clinical trials participants [55]. It is largely unknown whether these vaccines are safe and provide immunological protection in MS patients under specific DMDs, specifically those under B cell depleting therapies. Antiviral antibodies, notably those targeting the receptor binding domain of the viral spike protein, neutralize the virus and can contribute to the elimination of the primary SARS-CoV-2 infection in humans [56▪,57]. As B cells are required for the development of humoral immune responses to neoantigens there is a significant plausible risk that anti-CD20 therapies may diminish the future efficacy of a vaccine against SARS-CoV-2. However, B cells do not appear to be an absolute requirement for recovery in natural infection [58▪]. A greater understanding of the role of potential T cell responses induced by the covid vaccine and its effect on protection against SARS-CoV-2 infection will be decisive.
In shaping the best vaccination strategy for MS patients under B cell depleting therapies it will soon be time to consider the potential benefit of the ‘window for vaccination.’ It will require looking at the repopulation kinetics and introducing extended interval dosing or dosing interruption to allow immature B cells to recover. This strategy could be particularly suitable if anti-CD20 therapy is not urgent, potentially dispensable or replaceable with alternative therapies. Different MS societies recommend that the treatment decision-making process should weigh the benefits of DMDs for the individual patient versus the expected response to the SARS-CoV-2 vaccine. Current CDC recommends that immunocompromised individuals may receive COVID-19 vaccination if they have no additional contraindications. These patients should be counseled about the unknown vaccine safety profile and effectiveness in immunocompromised populations. Information about the potential for reduced immune responses and the need to continue following all currently recommended personal protective measures against COVID-19 should also be provided. In the absence of a valid correlate of protection, antibody testing is not recommended following mRNA COVID-19 vaccination and re-vaccination is not recommended after immune competence is regained. Eventually, as for other vaccines, it is not recommended to performed the injection during the very active phase of the disease or after high doses of corticosteroids [55].
CONCLUSION
Over the past years the MS field has witnessed an expansion of therapeutic options. Individualized therapy must now balance considerations of efficacy and side effects. A set of preventive strategies should be incorporated, including vaccination, into the algorithm of disease management to minimize risk of infection in individuals with MS. An early assessment of immunization needs will allow an optimization of vaccine response and avoid potential interference with treatment plans. Vaccinations are safe and effective for MS patients but some specific considerations should be kept in mind when planning vaccination strategies before, during and after receiving immunotherapy. Patients under immunosuppression and specifically B cell-depleting therapies are at risk of diminished immunogenicity to vaccines with relevant implications in the upcoming mass vaccination against SARS-CoV-2. Further understanding of vaccine response dynamics in MS patients under specific therapies, such as specific T cell responses even in the absence of neutralizing antibodies, will be crucial in order to shape the best vaccination strategy.