Physical Fitness Assessment

Selected By
June Halper, MSN, APN-C, MSCN, FAAN
Why is this important to me?
Participation in physical exercise can improve your walking ability, reduce your fatigue, and improve your quality of life. Conversely, being sedentary can result in loss of independence and reduced quality of life. Because MS is such a variable disease, your healthcare provider can provide a careful assessment of your physical ability and help to design the right exercise program for you. If you have some motor difficulty, a healthcare professional may be able to guide your choice of exercise equipment to ensure that you gain the most benefit from using it. This article discusses the authors' recommendations regarding the devices that will most accurately assess your level of physical ability and, therefore, the most appropriate exercise regime for you.
Who will benefit from reading this study/article?
Readers who seek to improve their quality of life and physical abilities with exercise, will benefit from reading this article.
What is the objective of this study?
This study compared two methods of assessing aerobic capacity and two methods for testing muscle strength. Aerobic capacity was assessed with arm ergometry, in which the person pedals a bike-like machine with their arms, and recumbent stepping, in which the participant uses a step machine while lying in a reclined position. Leg muscle strength was assessed with either a hand-held or computerized device. People with MS who participated were also assessed for disability, cognition, walking speed, fatigue, quality of life, and activities of daily living.
Arm cycle ergometry, in which the user "pedals" with their arms, has been used to assess aerobic capacity in people with moderate MS. However, because most of us have smaller muscle mass in our upper body, arm cycle ergometry can underestimate aerobic capacity by about 20 to 30%. A more accurate choice, especially for individuals with some mobility impairment, is a total body recumbent stepper. This is the first time that the recumbent stepper has been tested in patients with MS.
Muscle strength is commonly assessed in individuals with mobility impairment by using a device called a hand-held dynamometer. Here again, a better choice for detecting strength deficits is computerized dynamometry. Although computerized dynamometry has been used to identify strength deficits in people with mild to moderate disability, it has not been tested in individuals with advanced MS. The choice of device is therefore important in obtaining an accurate assessment of physical fitness in people with MS.
In addition to their aerobic capacity and muscle strength, participants in the study were observed for the impact of:
- Upper body sway while standing
- Varying levels of fatigue
- Cognition
- Level of daily activity
- Walking ability
- Quality of life
Your healthcare provider can work with you to establish a fitness program that is appropriate to your fitness level and ability. The results of this study suggest that the choice of devices used to measure your fitness level is important in developing a program that best meets your needs.
How did the authors study this issue?
The authors investigated 64 people with MS with a wide range of disability as measured by the Expanded Disability Status Scale. The average age of participants was 52 years, and 72% were female. Participants used both the arm pedaling machine and the step machine for determination of aerobic capacity, and both the hand-held and computerized devices for determination of leg muscle strength. The following parameters were also assessed in all participants:
- Disability
- Cognition
- Walking speed and endurance
- Postural sway
- Body composition
- Quality of life
- Activities of daily living
| SHARE: | |||||
Original Article
Physical Fitness Assessment Across the Disability Spectrum in Persons With Multiple Sclerosis: A Comparison of Testing Modalities
Journal of Neurologic Physical Therapy
Lara A. Pilutti, PhD, Brian M. Sandroff, MS, Rachel E. Klaren, BS, Yvonne C. Learmonth, PhD, Matthew E. Platta, BS, Elizabeth A. Hubbard, MS, Michelle Stratton, BS, and Robert W. Motl, PhD
INTRODUCTION
Exercise training can result in a number of benefits for individuals with multiple sclerosis (MS), such as improved walking, fatigue, quality of life, and chronic disease risk profile.1−3 Conversely there is evidence that sedentary behavior in persons with MS is associated with loss of independence and compromised health-related quality of life (HRQOL).4 The effects of exercise training depend upon an adequately designed training stimulus and adaptations in physical fitness (ie, cardiorespiratory fitness and muscular strength).5
Cardiorespiratory fitness and muscular strength have not been extensively or adequately evaluated in persons with advanced MS (ie, Expanded Disability Status Scale [EDSS] ≥ 6.0). This is likely due to the challenges of assessing physical fitness in persons with severe mobility impairment, such as physical inaccessibility of commonly used exercise modes (eg, walking on a treadmill).6 Accordingly, appropriate and physically accessible fitness assessment modalities are essential for optimal design and evaluation of exercise training interventions across the disability spectrum in MS.
Cardiorespiratory fitness has commonly been assessed in clinical populations with mobility impairment, such stroke and spinal cord injury, using arm cycle ergometry.7,8 Arm ergometry is a viable method for evaluating aerobic capacity and has been used in persons with moderate MS.9 Unfortunately, arm ergometry testing routinely underestimates peak aerobic capacity in both healthy and clinical populations by approximately 20% to 30,11 because of the use of a smaller muscle mass and, therefore, does not provide an accurate assessment of aerobic fitness. An alternative mode for persons with mobility impairment is a total body recumbent stepper. Recumbent stepping has been recommended by the American College of Sports Medicine for evaluating cardiorespiratory fitness in persons with neurologic disorders.12 Recumbent stepping has been established as a feasible, valid, and reliable mode for assessing aerobic capacity in healthy populations and stroke.13,14 However, recumbent stepping has not been adequately tested in MS.
Maximal muscle strength is commonly assessed in the clinical setting with persons with mobility impairment by manual muscle testing with or without a hand-held dynamometer.15,16 Manual muscle testing has good reliability and validity in persons with neuromuscular dysfunction16; however, the sensitivity of this method for detecting strength deficits has been challenged.17,18 An alternative modality is computerized dynamometry. Computerized dynamometry provides an objective and precise method for assessing strength in healthy and diseased populations and has superior sensitivity compared with manual approaches.17,18 Computerized dynamometry has been used to identify strength deficits in persons with MS who have mild to moderate disability,19,20 but not in persons with advanced MS.
This study involved a comparative evaluation of different modalities for measuring cardiorespiratory fitness (arm ergometry vs recumbent stepping) and muscular strength (hand-held dynamometer vs computerized dynamometer) across the disability spectrum in persons with MS. The study objectives were to determine (1) if the response to cardiorespiratory fitness and muscular strength testing differed between testing modes, (2) if the exercise response differed by MS disability level, and (3) if the relationship between physical fitness and other measures representing all domains of the International Classification of Functioning, Disability and Health (ICF) differed by the type of testing modality. Such an investigation represents an important first step in identifying best practices for the assessment of physical fitness across the disability spectrum in MS.
METHODS
Participants
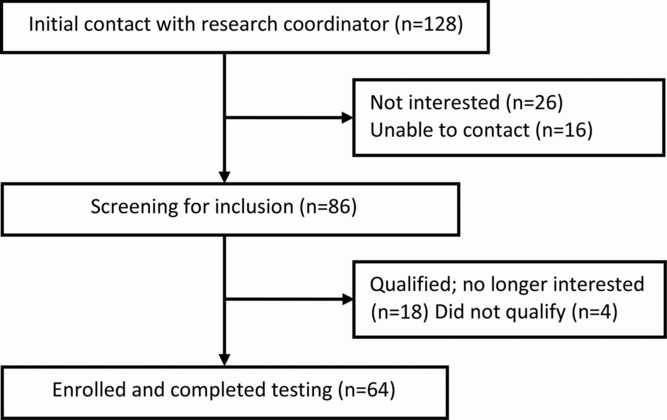
Participant recruitment was through distribution of flyers to participants within the North American Research Committee on Multiple Sclerosis registry and to participants from previous studies from our laboratory who had expressed interest in future research opportunities. Participant recruitment occurred between February 2013 and September 2013. Criteria for inclusion were physician-confirmed diagnosis of MS, 18 to 64 years of age, EDSS score less than 8.0, able to visit our laboratory on 2 testing occasions, minimal risk for engaging in physical activity (ie, reported “yes” to <2 questions on the Physical Activity Readiness Questionnaire),21 and physician approval. An equivalent number of participants with mild, moderate, and severe disability were recruited. Screening for initial disability status was performed via telephone using the self-reported EDSS.22 A detailed description of participant recruitment and enrollment is presented in Figure 1.
MS-Related Disability
Disability
Disability status was determined through a clinically administered EDSS23 examination by Neurostatus-certified assessors. Participants were grouped on the basis of the clinically determined EDSS score (ie, mild = EDSS 1.0-3.5; moderate = EDSS 4.0-5.5; severe = EDSS 6.0-7.5).
Fitness Measures
Aerobic Capacity (V˙ O2peak)
Aerobic capacity was assessed using an incremental exercise protocol with an arm ergometer (Ergometrics 800 arm ergometer; Ergoline, Lindenstrasse, Germany) and a recumbent stepper (Nustep T5XR recumbent stepper; Nustep Inc, Ann Arbor, Michigan). The same protocol was used for both aerobic exercise modes and was developed on the basis of exercise testing in persons with spinal cord injury.7 Expired gases were collected using a 2-way nonrebreathable valve (Hans Rudolph Inc, Shawnee, Kansas) and oxygen consumption was continuously measured using an open circuit spirometry system (TrueOne 2400, Parvo Medics, Sandy, Utah). Participants completed a 1-minute warmup at 15W. The initial work rate was set to 15W and was gradually increased until the participant reached volitional fatigue. The work rate increased by 10W per minute and 5W per minute for participants with mild to moderate and severe disability, respectively. Heart rate (Polar Electro Oy, Kempele, Finland) and rating of perceived exertion were recorded every minute. V˙ O2peak, expressed in mL/kg/min, was determined as the highest recorded 20-second V˙ O2 value when at least 1 of the following criteria was satis- fied: (1) respiratory exchange ratio 1.10 or greater; (2) peak heart rate within 10 beats per minute of age-predicted maximum (ie, 220-age); or (3) rating of perceived exertion 17 or greater.
Figure 1. Flow diagram of participant recruitment and enrollement.
Muscular Strength
Peak torque of the knee extensors (KE) and knee flexors (KF) was assessed bilaterally using a hand-held dynamometer (Lafayette Manual Muscle Testing System; Lafayette Instrument Company, Lafayette, Indiana) and a computerized dynamometer (Biodex System 3 Dynamometer; Biodex Medical Systems, Inc, Shirley, New York). Testing of the KE by handheld dynamometry was performed with participants seated with the hip flexed at 90◦ and knee flexed at 60◦. Testing of the KF by hand-held dynamometry was performed with participants lying in the prone position with the hip positioned at 180◦ and the knee flexed at 60◦. Knee flexor testing in the prone position was selected to allow for optimal positioning of the hand-held dynamometer and assessor. For each muscle group, participants performed three 5-second maximal voluntary contractions, with a 5-second rest between each attempt. A researcher stabilized the hand-held dynamometer by providing resistance against the contraction.24 Peak force per limb, expressed in newton (N), was determined as the highest recorded value for each muscle group, and converted to a measure of peak torque, expressed in newton meters (N·m). Knee extensor and KF peak torque was assessed by computerized dynamometry with participants seated on the dynamometer with the hip and knee flexed at 90◦ and 60◦, respectively. Participants performed three 5-second maximal KE and one 5-second maximal KF.25 There was a 5-second rest period between each attempt. Peak isometric strength, expressed in N·m, was determined as the highest recorded value for each muscle group. For both testing modalities, peak torque was expressed as an overall average of the 2 limbs for the KE and the KF.
ICF Domain Specific Measures
We examined the relationship between physical fitness and key areas of MS disability. The measures were grouped into body functions, activities, and participatory measures according to the World Health Organization ICF Framework.26 Measures were selected on the basis of expected relationships with fitness parameters (ie, walking endurance is likely correlated with aerobic capacity, whereas walking speed is likely correlated with muscular strength).5
Body Functions
Body functions involved measures of body composition, postural sway, cognition, and fatigue. Body composition was assessed by DXA using a Hologic QDR 4500A bone densitometer (software version 11.2, Hologic, Inc, Bedford, Massachusetts). Accuracy of the densitometer was verified by scanning the manufacturer’s hydroxyapatite spine phantom of a known density. Postural sway was assessed as center-ofpressure motion detected by a force platform (Bertec Corporation, Columbus, Ohio). Participants stood without shoes on the force platform for two 30-second trials. Data collected from the 2 trials were quantified as the amount of center-of-pressure motion indexed with sway area (based on a 95% confidence ellipse area) and velocity of postural sway along the anteroposterior and mediolateral axes.25 An average of the 2 trials was computed. Cognitive processing speed was assessed using the Symbol Digit Modalities Test.27 The impact of fatigue was assessed using the 21-item Modified Fatigue Impact Scale.28
Activities
Activities involved walking speed and endurance. Walking speed was assessed using the Timed 25-foot Walk and was administered according to standardized instructions.29 Walking endurance was assessed using the 6-minute walk test.30 A member of the research team followed 1 to 3 m behind the participant with a measuring wheel (CST Berger, Stanley MW50, New Briton, Connecticut) to quantify the total distance walked in meters.
Participation
Participatory measures included HRQOL and activities of daily living (ADL). Physical and psychological HRQOL were assessed using the 29-item Multiple Sclerosis Impact Scale (MSIS-29).31 The functional limitations component of the abbreviated Late Life-Function and Disability Inventory (LL-FDI) was used as a measure of ADL.32 Procedures All procedures were approved by the University of Illinois at Urbana–Champaign institutional review board and participants provided written informed consent. Participants completed 2 testing sessions separated by approximately 1 week. All testing took place at a university research laboratory between April 2013 and October 2013. At the first testing session, participants underwent the neurological examination. At each testing session, participants completed 1 cardiorespiratory fitness test and 1 muscular strength test. The fitness tests were administered in a counterbalanced order across testing sessions. The remaining measures were distributed between the 2 testing days. The test order provided a balance between active and nonactive tests to minimize participant fatigue. Each testing session took approximately 120 minutes to complete and participants received $75.
Data Analysis
Statistical analyses were performed using SPSS (Version 22.0; SPSS Inc, Chicago, Illinois). Descriptive statistics were used to summarize demographic and clinical characteristics. Values are presented in the text as mean (SD), unless otherwise noted. To compare fitness test measures across the disability spectrum, a mixed-model analysis of variance (ANOVA) with testing mode as a within-subjects factor and disability level as a between-subjects factor was performed. The reliability of the fitness tests was examined overall and by disability level using a 2-way mixed-effect model for determining intraclass correlation coefficients (ICC). Bland-Altman33 plots were generated to examine overall and systematic differences in peak fitness between the testing modalities. The relationship between physical fitness and body functions, activities, and participatory measures was examined using Pearson product-moment (r) correlations. Correlations coefficients of 0.1, 0.3, and 0.5 were interpreted as small, moderate, and large, respectively.34 The significance of the difference in correlation coefficients between testing modalities was compared using the Steiger Z test for paired correlations.35 Statistical significance was set a P < 0.05. Missing cases were not included in data analyses. Missing data occurred for fitness measures (n = 0-4) and other measures (n = 1-8).
RESULTS
Participant Characteristics
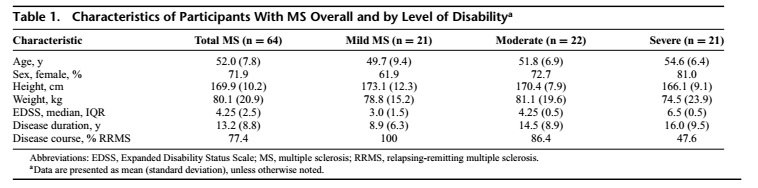
Demographic and clinical characteristics of the overall sample and by disability group are presented in Table 1. There were no differences between disability groups in age (P = 0.13), height (P = 0.08), weight (P = 0.55), or sex (P = 0.39). There was a significant difference in disease duration between disability groups (P = 0.02). Participants with severe MS reported longer disease duration than those with mild MS. There was a significant difference in disease course by disability group (P < 0.001); participants with mild and moderate MS had predominately a relapsing disease course, whereas participants with severe MS had an equal distribution of relapsing and progressive disease courses.
Physical Fitness Disability
Aerobic Capacity
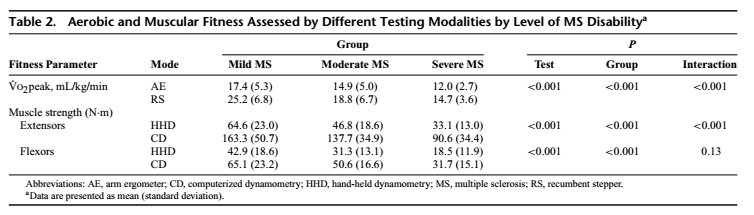
Peak aerobic capacity assessed by recumbent stepping was higher when compared with arm ergometry (F1,59 = 117.79, P < 0.001, ηρ2 = 0.66; Table 2). Overall, peak aerobic capacity decreased as a function of increasing disability (F2,59 = 13.58, P < 0.001, ηρ2 = 0.32). There was a significant interaction between aerobic capacity test modality and disability (F2,59 = 10.49, P < 0.001, ηρ2 = 0.26), and this indicates that the difference in peak aerobic capacity measured by the 2 test modes was largest for the mild group and smallest for the severe group.
Muscular Strength
With respect to KE, peak torque was significantly higher when assessed by computerized dynamometry compared with hand-held dynamometry (F1,60 = 386.93, P < .001, ηρ2 = 0.87) (Table 2). The KE strength decreased as a function of increasing disability (F2,60 = 19.32, P < 0.001, ηρ2 = 0.39). There was a significant interaction between strength test modality and disability (F2,60 = 9.13, P < 0.001, ηρ2 = 0.23), and this indicates that the difference in peak torque measured by the 2 test modes was largest for the mild group and smallest for the severe group. Regarding KF, peak torque was significantly higher when assessed by computerized dynamometry compared with hand-held dynamometry (F1,60 = 101.19, P < 0.001, ηρ2 = 0.63). The KF strength decreased as a function of increasing disability (F2,60 = 18.51, P < 0.001, ηρ2 = 0.38). There was no significant interaction between strength testing mode and disability for KF.
Reliability and Agreement of Fitness Tests
Aerobic Capacity
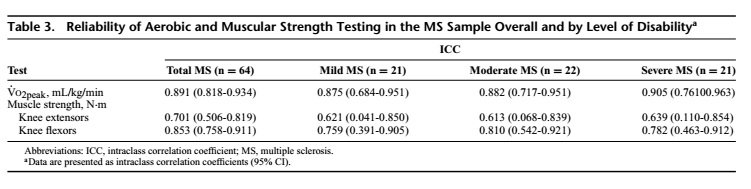
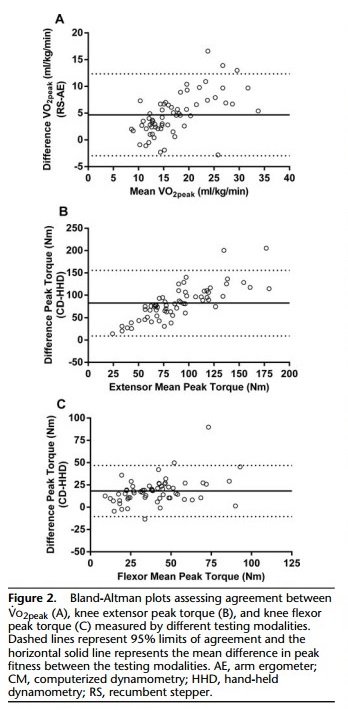
The ICC for aerobic capacity was 0.891 in the overall sample and was more than 0.8 in all disability groups (Table 3), suggesting good agreement in rank ordering across the disability spectrum.36 The Bland-Altman plot for aerobic capacity indicates that the differences in peak fitness between testing modalities were generally within 2 SD (Figure 2). There was a mean difference of 4.7 (3.91) mL/kg/min in peak aerobic capacity between testing modes. The differences in peak aerobic capacity varied systematically by fitness level; differences were greatest for individuals with the highest aerobic fitness. Muscular Strength The ICC for KE testing was 0.701 (Table 3) and this indicates moderate reliability overall.36 The ICC for KF testing was 0.853 in the overall sample, suggesting good reliability.36
The differences in peak fitness between testing modalities were generally within 2 SD based on Bland-Altman plots (Figure 2). There was a mean difference of 82.4 (37.4) N·m in peak torque for KE and a mean difference of 18.2 (14.6) N·m in peak torque for KF. The differences in peak torque of the KE were greatest for individuals with the highest peak torque. There did not appear to be systematic variation in peak torque differences for KF.
Physical Fitness and ICF Domain Specific Measures
Aerobic Capacity
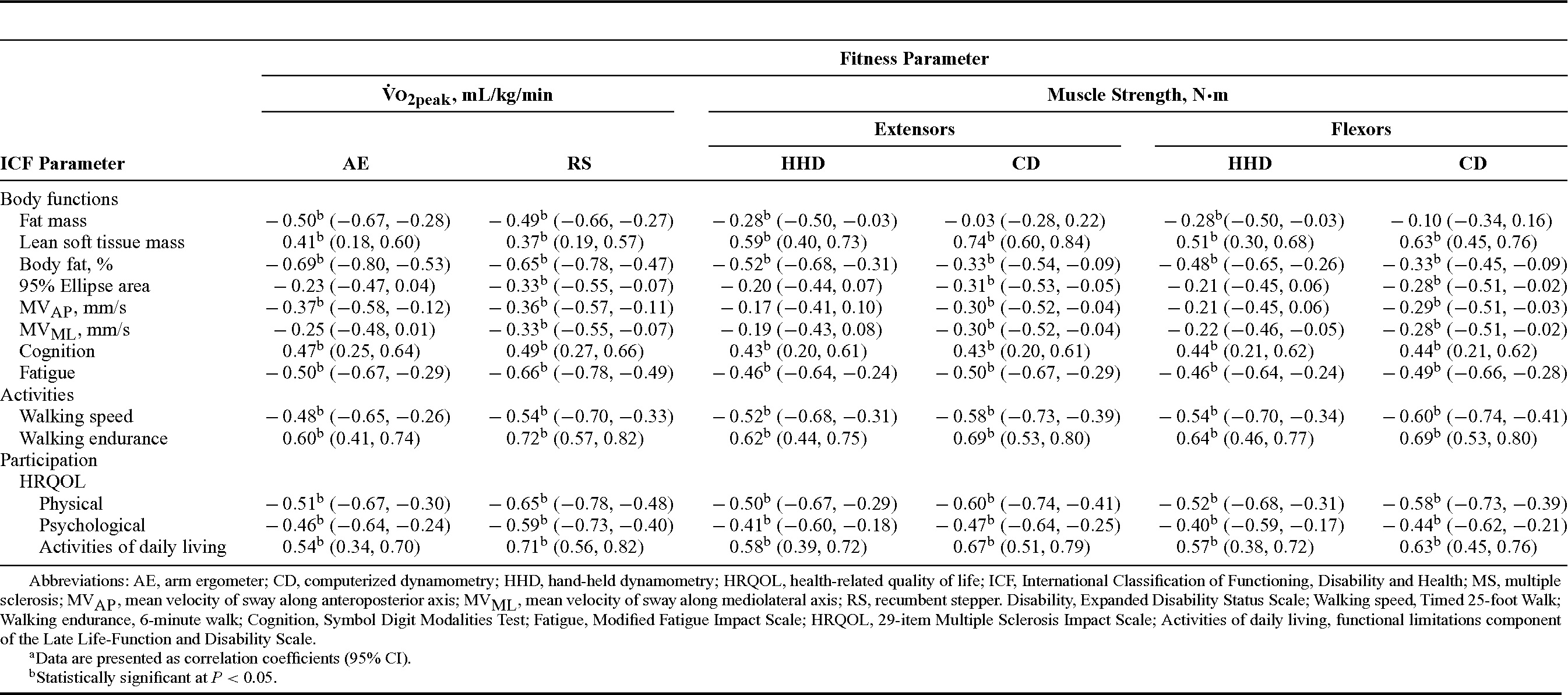
With respect to body functions, there were significant, moderate to strong correlations between aerobic capacity and all body composition measures (r = ||0.37-0.69||; Table 4). Significant, small to moderate correlations were observed between aerobic capacity assessed using the recumbent stepper and all postural sway metrics (r = −0.34 to −0.37). Only the relationship between aerobic capacity based on arm ergometry and mediolateral postural sway was statistically signifi- cant (r = −0.38). Significant, moderate to strong correlations were observed between aerobic capacity and cognition and fatigue (r = ||0.47-0.66||) using both test modalities. Moderate to strong correlations were observed between aerobic capacity and activities (r = 0.48-0.72) and participatory measures (r = ||0.46-0.71||) with both testing modes. Aerobic capacity assessed on the recumbent stepper was more strongly associated with ADL than aerobic capacity assessed using the arm ergometer (P = 0.001). There were no other significant differences in correlation coefficients between aerobic capacity testing modalities and any other measures.
Muscular Strength
Regarding body functions, significant, small correlations were observed between muscle strength assessed by hand-held dynamometry and fat mass (r = −0.28; Table 4). There were no significant relationships between muscle strength based on computerized dynamometry and fat mass. There were significant correlations between muscle strength and lean mass and percent body fat, assessed using both modes; the correlations were generally moderate to strong in magnitude (r = ||0.33-0.74||). Small to moderate correlations were observed between muscle strength and postural sway assessed using both modes (r = −0.17 to −0.31). Significant, moderate to strong correlations were observed between muscle strength and cognition and fatigue (r = ||0.43-0.50||) with both test modalities. There were moderate to strong correlations observed between aerobic capacity and activities (r = 0.52- 0.69) and participatory measures (r = ||0.40-0.67||) using both testing modes. None of the correlation coefficients were significantly different between the strength testing modalities and other measures.
DISCUSSION
This study involved a comparative, cross-sectional investigation of different modalities for assessing cardiorespiratory fitness and muscular strength across the disability spectrum in persons with MS. Overall, peak aerobic capacity, KE peak torque, and KF peak torque were 32%, 173%, and 60% greater, respectively, on the basis of recumbent stepping and computerized dynamometry testing. This suggests that the determination of peak fitness and prescription of exercise training in MS should be based on these testing modalities. There were no differences in the associations between physical fitness and body functions, activities, and participatory measures between the testing modalities. This suggests that an important association exists between physical fitness and other measures in MS, regardless of the fitness assessment modality.
Peak aerobic capacity and peak torque were underestimated when assessed by arm ergometry and hand-held dynamometry testing, respectively. This is not surprising considering that peak aerobic performance is known to be reduced with upper body exercise compared with lower body exercise.10,11 Several physiological factors are believed to be contribute to reduced upper body performance including a smaller and weaker muscle mass, inadequate blood perfusion, and reduced oxidative capacity of the upper extremities.11 Furthermore, maximal strength assessed by hand-held dynamometry is greatly limited by the strength and body mass of the assessor,37 whereas computerized dynamometry testing maintains the participants’ limb in a fixed position. The difference recorded in peak fitness has important implications for exercise prescription. For example, if aerobic exercise was prescribed at an intensity of 60% V˙ O2peak, this would result in a substantially different workload if the prescription was based on cardiorespiratory testing using an arm ergometer compared with a recumbent stepper. This suggests that the prescription of exercise training should be based on recumbent stepping and computerized dynamometry whenever possible, rather than arm ergometry or hand-held dynamometry, to ensure an adequate training stimulus to maximize beneficial physiological adaptations. Alternatively, hand-held dynamometry testing might be improved through the addition of a stabilization strap in clinical settings without access to computerized dynamometry.
In this study, a relationship was observed between physical fitness and disability, such that participants with more severe impairment had reduced aerobic capacity and muscular strength. This corroborates results from previous reports that suggest persons with MS with worse disease burden have greater mobility disability and limited capacity for participating in physical activity, which, in turn, might contribute to physiological deconditioning.2,5 Previous studies have demonstrated cross-sectional associations between EDSS scores and aerobic capacity assessed by arm or leg ergometry,9,38 and differences in aerobic capacity between persons with mild (EDSS = 1.0-4.5) and moderate to severe (EDSS = 5.0-6.5) MS assessed by leg ergometry.39 Collectively, these findings highlight the need for targeted interventions that improve and restore physical fitness, particularly in persons with advanced MS who experience the greatest physiological deconditioning, and wherein pharmacological management has limited efficacy.40,41
Regarding reliability of the fitness tests, good reliability overall and across the disability spectrum was determined for both aerobic test modalities. In healthy controls, aerobic capacity assessed by recumbent stepping and a Bruce protocol treadmill test also demonstrated high reliability.13 Hand-held dynamometry and computerized dynamometry had moderate reliability for KE strength and good reliability for KF strength in the overall MS sample. It is challenging to accurately assess muscle strength by hand-held dynamometry due to limitations in the ability to stabilize the hand-held device. This task can be more challenging when assessing the KE. Indeed, the magnitude and reliability of hand-held dynamometry measurement are greatly reduced at forces beyond 120 N.37 The strength difference between KE and KF likely contributed to the difference in test reliability observed between these muscle groups.
While moderate to good reliability for the fitness tests was established, there was a lack of agreement in peak fitness. Peak fitness was underestimated using arm ergometry and hand-held dynamometry compared with recumbent stepping and computerized dynamometry testing, respectively. The differences in peak fitness further varied systematically for aerobic capacity and muscular strength of KE, such that the differences were greatest for individuals with the highest fitness. This is not surprising considering the extremely low level of cardiorespiratory fitness and limited exercise capacity in the severe MS group. This provides important information regarding the potential for discrepancies in peak fitness between testing modalities and further highlights the need for assessment modalities that accurately assess physical fitness across the disability spectrum in MS.
Overall, there were significant, moderate to strong correlations between both cardiorespiratory fitness and muscular strength measures and body functions, activities, and participatory measures. The correlation coefficients were similar in magnitude between the different cardiorespiratory fitness and muscular strength test modalities. Similar relationships have been established in other MS samples.9,25,42,43 For instance, one study reported that aerobic capacity (based on cycle ergometry) and muscle strength asymmetries (based on computerized dynamometry) were significantly correlated with walking speed, walking endurance, and spatiotemporal gait parameters in 31 persons with MS (median PDDS = 2.0).43 Collectively, this suggests an important relationship between physical fitness and other measures in MS, regardless of fitness testing mode.
Limitations
Fitness modes other than those we assessed (eg, cycle ergometry) could have been evaluated and might have resulted in different relationships than those observed in this study. Although a variety of body functions, activities, and participatory measures were included, there are additional measures that could have been assessed. For instance, fatiguewas selected as a measure of mental body functions since it is the most prevalent and disabling symptom experienced by persons with MS.44,45 Other mental body functions such as depression might also be important and might have different associations with physical fitness. We further note the difference in body position for KF strength assessment between the test modalities (ie, seated vs prone) as a potential limitation, although the angle of the knee was held constant. The results of this study are generalizable to individuals with MS of varying disability levels, but who are primarily female with a relapsing disease course.
CONCLUSIONS
This study involved the first comparison of different modalities for assessing cardiorespiratory fitness and muscular strength across the disability spectrum in MS. Peak aerobic capacity and peak torque were greater when assessed by recumbent stepping and computerized dynamometry, respectively, and decreased as a function of increasing disability. These results should inform the design and evaluation of the efficacy of exercise training with persons with a broad range of MS disability. Significant relationships between physical fitness and body functions, activities, and participatory measures were established, regardless of fitness testing modality. This emphasizes the importance of targeting cardiorespiratory fitness and muscular strength measures through therapeutic intervention in MS.
REFERENCES
1. Motl RW, Pilutti LA. The benefits of exercise training in multiple sclerosis. Nat Rev Neurol. 2012;8:487-497.
2. Latimer-Cheung AE, Pilutti LA, Hicks AL, et al. The effects of exercise training on fitness, mobility, fatigue, and health related quality of life among adults with multiple sclerosis: a systematic review to inform guideline development. Arch Phys Med Rehabil. 2013;94:1800-1828.
3. Dalgas U, Stenager E, Ingemann-Hansen T. Multiple sclerosis and physical exercise: recommendations for the application of resistance-, endurance- and combined training. Mult Scler. 2008;14:35-53.
4. Ellis T, Motl RW. Physical activity behavior change in persons with neurologic disorders: overview and examples from Parkinson disease and multiple sclerosis. J Neurol Phys Ther. 2013;37:85-90.
5. Motl RW, Pilutti LA, Sandroff BM. The importance of physical fitness in multiple sclerosis. J Nov Physiother. 2013;3:1000141.
6. Pilutti LA, Hicks AL. Role of exercise in multiple sclerosis: potential application of adapted exercise modalities. Crit Rev Phys Rehabil Med. 2011;23:175-194.
7. Pelletier CA, Jones G, Latimer-Cheung AE, Warburton DE, Hicks AL. Aerobic capacity, orthostatic tolerance, and exercise perceptions at discharge from inpatient spinal cord injury rehabilitation. Arch Phys Med Rehabil. 2013;94:2013-2019.
8. Sutbeyaz ST, Koseoglu F, Inan L, Coskun O. Respiratory muscle training improves cardiopulmonary function and exercise tolerance in subjects with subacute stroke: a randomized controlled trial. Clin Rehabil. 2010;24:240- 250.
9. Koseoglu BF, Gokkaya NK, Ergun U, Inan L, Yesiltepe E. Cardiopulmonary and metabolic functions, aerobic capacity, fatigue and quality of life in patients with multiple sclerosis. Acta Neurol Scand. 2006;114:261- 267.
10. McArdle WD, Katch FI, Katch VL. Exercise Physiology: Energy, Nutrition, and Human Performance. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001.
11. Sawka MN, Foley ME, Pimental NA, Pandolf KB. Physiological factors affecting upper body aerobic exercise. Ergonomics. 1983;26:639-646.
12. Durstine JL, Moore GE, Painer PL, Roberts SO, eds. ACSM: Exercise Management for Persons With Chronic Diseases and Disabilities. 3rd ed. Champaign, IL: Human Kinetics; 2003.
13. Billinger SA, Loudon JK, Gajewski BJ. Validity of a total body recumbent stepper exercise test to assess cardiorespiratory fitness. J Strength Cond Res. 2008;22:1556-1562.
14. Billinger SA, Tseng BY, Kluding PM. Modified total-body recumbent stepper exercise test for assessing peak oxygen consumption in people with chronic stroke. Phys Ther. 2008;88:1188-1195.
15. Hislop H, Montgomery J. Daniel and Worthingham’s Muscle Testing: Techniques of Manual Examination. 8th ed. Philadelphia, PA: Saunders Elsevier; 2007. 16. Cuthbert SC, Goodheart GJ On the reliability and validity of manual muscle testing: a literature review. Chiropr Osteopat. 2007;15:4.
17. Bohannon RW. Manual muscle testing: does it meet the standards of an adequate screening test? Clin Rehabil. 2005;19:662-667.
18. Bohannon RW. Manual muscle testing overlooks many knee extension strength deficits among older adults. Isokinet Exerc Sci. 2010;18: 185-187.
19. Lambert CP, Archer RL, Evans WJ. Muscle strength and fatigue during isokinetic exercise in individuals with multiple sclerosis. Med Sci Sports Exerc. 2001;33:1613-1619.
20. Ponichtera JA, Rodgers MM, Glaser RM, Mathews TA, Camaione DN. Concentric and eccentric isokinetic lower extremity strength in persons with multiple sclerosis. J Orthop Sports Phys Ther. 1992;16: 114-122.
21. Thomas S, Reading J, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can J Sport Sci. 1992;17:338-345.
22. Ratzker PK, Feldman JM, Scheinberg LC, et al. Self-assessment of neurologic impairment in multiple sclerosis. Neurorehabil Neural Repair. 1997;11:207–211.
23. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an Expanded Disability Status Scale (EDSS). Neurology. 1983;33:1444-1452.
24. Bohannon RW. Measuring knee extensor muscle strength. Am J Phys Med Rehabil. 2001;80:13-18.
25. Sandroff BM, Motl RW. Fitness and cognitive processing speed in persons with multiple sclerosis: a cross-sectional investigation. J Clin Exp Neuropsychol. 2012;34:1041-1052.
26. International Classification of Functioning, Disability and Health. World Health Organization Web site: http://www.who.int/classifications/icf/en./. Published 2001. Updated October 17, 2014. Accessed February 27, 2015.
27. Smith A. Symbol Digit Modalities Test: Manual. Los Angeles, CA: Western Psychological Services; 1982.
28. Fisk JD, Ritvo PG, Ross L, Haase DA, Marrie TJ, Schlech WF. Measuring the functional impact of fatigue: initial validation of the Fatigue Impact Scale. Clin Infect Dis. 1994;18:S79-S83.
29. Fischer JS, Jak AJ, Knicker JE, Rudick RA, Cutter GI. Administration and Scoring Manual for the Multiple Sclerosis Functional Composite Measure (MSFC). New York, NY: Demos Medical Publishing Inc; 1999.
30. Goldman MD, Marrie RA, Cohen JA. Evaluation of the six-minute walk in multiple sclerosis subjects and healthy controls. Mult Scler. 2008;14:383- 390. 31. Hobart J, Lamping D, Fitzpatrick R, Riazi A, Thompson A. The Multiple Sclerosis Impact Scale (MSIS-29): a new patient-based outcome measure. Brain J Neurol. 2001;124:962-973.
32. McAuley E, Konopack JF, Motl RW, Rosengren K, Morris KS. Measuring disability and function in older women: psychometric properties of the late-life function and disability instrument. J Gerontol A Biol Sci Med Sci. 2005;60:901-909.
33. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307-310. 34. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988.
35. Steiger JH. Tests for comparing elements of a correlation matrix. Psychol Bull. 1980;87:245-251.
36. Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to Their Development and Use. London, UK: Oxford University Press; 2008.
37. Wikholm JB, Bohannon RW. Hand-held dynamometer measurements: tester strength makes a difference. J Orthop Sports Phys Ther. 1991;13:191-198
38. Motl RW, Goldman M. Physical inactivity, neurological disability, and cardiorespiratory fitness in multiple sclerosis. Acta Neurol Scand. 2011;123:98-104.
39. Ponichtera-Mulcare JA, Mathews T, Barrett PJ, Gupta SC. Change in aerobic fitness of patients with multiple sclerosis during a 6-month training program. Sports Med Train Rehabil. 1997;7:265-272.
40. Brown T, Kraft GH. Exercise and rehabilitation for individuals with multiple sclerosis. Phys Med Rehabil Clin N Am. 2006;16:513-555.
41. Motl RW. Physical activity and irreversible disability in multiple sclerosis. Exerc Sport Sci Rev. 2010;38:186-191.
42. Broekmans T, Gijbels D, Eijnde BO, et al. The relationship between upper leg muscle strength and walking capacity in persons with multiple sclerosis. Mult Scler J. 2013;19:112-119.
43. Sandroff BM, Sosnoff JJ, Motl RW. Physical fitness, walking performance, and gait in multiple sclerosis. J Neurol Sci. 2013;328: 70-76.
44. Freal JE, Kraft GH, Coryell JK. Symptomatic fatigue in multiple sclerosis. Arch Phys Med Rehabil. 1984;65:135-138.
45. Bakshi R. Fatigue associated with multiple sclerosis: diagnosis, impact and management. Mult Scler. 2003;9:219-227.
