Effects of a Cognitive Behavioral Program for Women with MS

Selected By
June Halper, MSN, APN-C, MSCN, FAAN
Why is this important to me?
When faced with the diagnosis of MS, patients are forced into a new reality and must learn to cope with related stress factors that come with the progression of the disease. Stressful life events have been linked to exacerbations. Dealing with daily life stressors such as uncertainty about the future, functional and cognitive impairments, fatigue and difficulties maintaining a job can contribute to depression and mood swings.
“Beyond MS” explored the importance for psychosocial intervention to help patients learn how to cope with emotional challenges they face when dealing with the disease progression. The program also fostered individual goal setting to help participants enhance their self-confidence. Participants in the program not only gained a sense of community and self-assurance, the counselors saw significant improvements in perceived health competence, coping behaviors, and a variety of psychological outcomes experienced by the participants. “Beyond MS” enforced the age-old mantra to “accept the things you cannot change, the courage to change the things you can, and the wisdom to know the difference.”
What was the objective of this article?
A cognitive-behavioral study, “Beyond MS”, was conducted to enhance perceived control of patients meeting on a weekly basis in a group setting. The study was done to help patients develop coping skills as well as assess the psychological and physical outcomes.
How did the authors study this issue?
Thirty-seven women with MS participated in a group-based program led by psychiatric nurses.The program involved reading a manual and meeting for a weekly discussion for five consecutive weeks. The participants’ health competence, coping behaviors, psychological well-being, quality of life and fatigue levels were measured five weeks prior to the program, immediately before the program, at the end of the program and again six months after the program concluded.
| SHARE: | |||||
Original Article
Effects of a Cognitive-Behavioral Program for Women with Multiple Sclerosis
Vaughn G. Sinclair, Jennifer Scroggie
Journal of Neuroscience Nursing
Abstract:
The purpose of this quasi-experimental study was to evaluate the effectiveness of a cognitive-behavioral intervention for women with multiple sclerosis (MS). Thirty-seven adult women with MS participated in a group-based intervention program titled “Beyond MS,” which was led by master’s-prepared psychiatric nurses. For participants, the program involved reading a manual and meeting for five weekly group sessions. Perceived health competence, coping behaviors, psychological well-being, quality of life, and fatigue were measured at four time periods: 5 weeks before the beginning of the intervention, immediately before the intervention, at the end of the 5-week intervention, and at a 6-month follow-up. There were significant improvements in the participants’ perceived health competence (p < .01), indices of adaptive and maladaptive coping (p < .04), and most measures of psychological well-being (p < .05) from pre- to postintervention. The positive changes brought about by this relatively brief intervention program were maintained during the 6-month follow-up period. This cognitive-behavioral intervention has also been used effectively in the rheumatoid arthritis population and may be adaptable to benefit individuals with other chronic conditions.
Multiple sclerosis (MS) is a chronic, progressive, demyelinating disease of the central nervous system. The current prevalence in the United States is approximately 350,000 (Holland, 2004), with an annual incidence of about 12,000 and initial onset typically occurring between the ages of 18 and 45 years (Frohman, 2003). Given the progressive nature of MS, individuals living with this condition must cope with substantial disease-related stress and the uncertainty of their future disease course.
Although the role of stress in triggering MS exacerbations has been debated for years, recent studies have established links between stressful life events and exacerbations (Ackerman et al., 2002; Buljevac et al., 2003; Mohr, Goodkin, Nelson, Cox, & Weiner, 2002; Mohr, Hart, Julian, Cox, & Pelletier, 2004). On a daily basis, persons with MS deal with significant stressors related to uncertainty about the future, functional and cognitive impairments, and general loss of control in their lives (Minden, 1992). After diagnosis, their greatest stressors include fatigue, uncertainty about the future, and difficulties in maintaining a job (Buelow, 1991). Researchers have also documented the experience of chronic sorrow, encompassing sadness, anger, frustration, fear, and helplessness, that surfaces when persons with MS feel out of control (Hainsworth, 1994; Minden, 1992). High levels of uncertainty about the future course of the illness and perceived stress have been correlated with mood disturbances in persons with MS (Kroencke, Denney, & Lynch, 2001; Wineman, Schwetz, Goodkin, & Rudick, 1996). Many individuals with MS become depressed, with point prevalence rates reported in the literature between 25% and 54% (Beatty, 1993; Chwastiak et al.; Murray, 1995; Schiffer, 1990). The depression may be partially caused by MS-specific processes, but a variety of psychosocial factors also can contribute to depression in this population (Mohr & Cox, 2001). The emotional component of this disease experience, therefore, presents complex and difficult challenges. There is a need for effective psychosocial interventions to help individuals with MS cope with the emotional challenges associated with living with the condition.
This article presents findings of a cognitive-behavioral intervention program for women with MS. The program was designed to enhance perceived control and thereby affect coping skills as well as psychological and physical outcomes.
Review of the Literature
The manner in which individuals handle their emotional challenges may affect the course of their disease. Perceptions of disease-related stressors, particularly uncertainty, affect coping behaviors that can, in turn, affect psychological outcomes (Brassington & Marsh, 1998; Wineman, Durand, & Steiner, 1994). Learned helplessness, the antithesis of perceived control, has been significantly correlated with both social and functional disability in persons with MS (McGuinness, 1996). Perceptions of helplessness have been associated with both neurological impairment and emotional instability and mediated the relationship between impairment and fatigue severity (Van der Werf, Evers, Jongen, & Bleijenberg, 2003).
Because MS entails daily uncertainty, confidence in one’s ability to rise to the challenge (i.e., self-efficacy) should help neutralize the stressor of unpredictability. A high level of perceived control, whether measured as internal locus of control, self-efficacy, mastery, or perceived health competence, has surfaced in the MS literature as a construct affecting psychological and physical outcomes. For persons with MS, an effective internal locus of control has been linked with positive psychosocial adjustment, less depression, an active personal life (Murray, 1995), and a more benign course of MS (Wassem, 1991). Self-efficacy represents a form of perceived control applied to specific challenges and has been a significant predictor of adjustment to MS (Wassem, 1992). After adjusting for sociodemographic and medical factors in their regression analyses, Schwartz, Coulthard-Morris, and Zeng (1996) reported that a low sense of mastery was the best psychosocial predictor of both global fatigue and fatigue-related distress. More severe fatigue was correlated with higher levels of depression in their sample. Self-efficacy has emerged as a significant predictor of health-promoting behaviors in individuals with MS (Stuifbergen & Becker, 1994), with subsequent impacts on quality of life, as demonstrated in a structural equation model of health promotion and quality of life derived from a sample of 786 individuals with MS (Stuifbergen, Seraphine, & Roberts, 2000). Gulick (2001) found that certain personal attributes (i.e., positive attitude, a sense of humor, perceived control over stress) mediated the effects of emotional distress on functionality in a large sample of 686 persons with MS. The psychosocial literature on MS therefore implies that psychosocial interventions for this population should focus on improving perceptions of control or self-efficacy.
Various approaches to psychosocial intervention have been attempted in this population. Support groups (Spiegelberg, 1980), medical discussion groups (Pavlou, Hartings, & Davis, 1978), extensive group psychotherapy (Crawford & McIvor, 1985; Hartings, Pavlou, & Davis, 1976), cognitive-behavioral therapy (CBT) groups (Foley & Bedell, 1987; Larcombe & Wilson, 1984), CBT delivered via reading a manual or conducting a telephone interview (Mohr et al., 2000), and coping-skills interventions (Schwartz, 1999; Schwartz & Rogers, 1994). Among these researchers, those who used some form of cognitivebehavioral intervention found them to be effective at significantly reducing depression levels (Crawford & McIvor; Foley & Bedell; Larcombe & Wilson; Mohr et al.), symptoms of depression (Mohr et al.), and anxiety and distress levels (Crawford & McIvor). Most of the samples were small (i.e., fewer than 30 participants per treatment group).
More recent interventions partially based on the behavioral principles of social cognitive theory (Bandura, 1986, 1998) have reported positive psychological and physical changes. Mathiowetz, Matuska, and Murphy (2001) used a 6-week energy conservation course in a quasi-experimental study in which 54 subjects served as their own controls. The researchers’ intervention resulted in significant improvements in fatigue impact, self-efficacy, and several aspects of quality of life (i.e., vitality, social functioning, mental health). Stuifbergen, Becker, Blozis, Timmerman, and Kullberg (2003) used a randomized controlled trial to assess the effectiveness of a wellness intervention program for women with MS. This program used an eight-session format to deliver health-promotion information and practice techniques, incorporate individualized goal setting and monitoring, and attempt to enhance self-efficacy for health behaviors. The intervention resulted in significant improvements in self-efficacy, health behaviors, and aspects of quality of life, including pain and mental health. In general, the interventions for persons with MS that have been based on cognitive-behavioral or behavioral principles have been most effective.
This article discusses findings of a pilot program of a cognitive-behavioral intervention titled “Beyond MS.” This intervention program was modeled after “Rising Above Arthritis” (subsequently renamed “Beyond Arthritis”), a program developed with funding from the Arthritis Foundation to help women with rheumatoid arthritis (RA) develop a sense of competence in dealing with both arthritis-related problems and other life stressors (Sinclair, Wallston, Dwyer, Blackburn, & Fuchs, 1998). In a sample of 90 women with RA, analysis of changes between pre- and postintervention averaged scores revealed significant improvement on all measures of personal coping resources (e.g., helplessness and perceived control [p < .001], adaptive and maladaptive pain coping behavior indices [p < .05], and all measures of psychological well-being [p < .05]). Furthermore, the positive changes brought about by the program were maintained during a 3-month follow-up period.
Both RA and MS are progressive, highly unpredictable autoimmune conditions. Both patient populations deal with stress related to uncertainty, disability, fatigue, pain, and dependence on others for assistance. The researchers therefore believed that a psychosocial program that had promising effects in a sample of women with RA merited investigation with a sample of women with MS.
The pilot study to modify the initial RA intervention and test its effects with women with MS was funded by the National Multiple Sclerosis Society, with initial program evaluation funding from the Middle Tennessee Chapter of the Multiple Sclerosis Society.
Conceptual Model
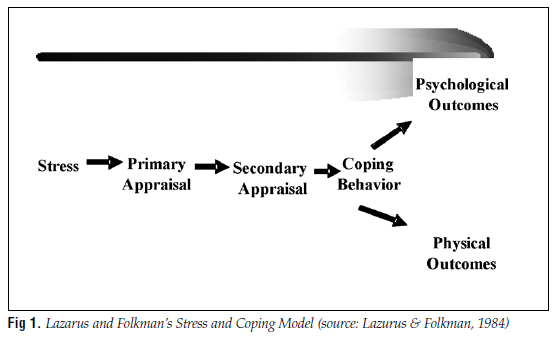
The Lazarus and Folkman Stress and Coping Model (Lazarus & Folkman, 1984) underscores the pivotal role perception plays in adaptation to stress. According to the model, individuals respond to stressors by appraising the potency of the stressor (the primary appraisal) and appraising their resources for meeting the challenge (the secondary appraisal). These two types of appraisal influence coping behaviors that affect psychological wellbeing and perceptions of quality of life. This model (Fig 1) indicates that an intervention designed to enhance a sense of perceived control or competence would positively affect appraisal mechanisms and thereby affect coping patterns and psychological outcomes. The “Beyond MS” program teaches cognitive means of making stressors seem less threatening and augments resources for meeting challenges by affecting appraisal mechanisms through a variety of strategies.
Hypotheses
Two hypotheses guided this research: (a) compared to preintervention scores, postintervention scores will reflect a positive impact on patients’ perceptions of competence, coping behaviors, psychological well-being, and healthrelated quality of life, and fatigue; and (b) compared to initial postintervention scores, 6-month follow-up scores indicating perceived health competence, coping behaviors, psychological well-being, health-related quality of life, and fatigue will reflect stabilization or improvement.
Methods
Sample
Following institutional review board approval of the protocol, the researchers recruited, with the help of local neurologists and the Middle Tennessee Multiple Sclerosis Society, a convenience sample of 47 women diagnosed by a neurologist with definite or probable MS. This pilot study sample size was small, so gender, stage of the disease, and degree of disability were controlled to limit variability caused by these potentially confounding variables. The inclusion criteria included female gender; relapsingremitting MS; and ambulatory Expanded Disability Status Scale (Kurtze, 1983) scores (less than 6). The women in this convenience sample voluntarily contacted the researchers. Six women withdrew from the study before the first session because of work conflicts, children requiring surgery, care of critically ill parents, or disease exacerbations. Four women withdrew after attending only one session. One of them had a debilitating back injury, one experienced an extreme exacerbation, and two found they were too fatigued to come to the weekly sessions. Thirty-seven women completed the program and provided postintervention data.
Because of limited funding for this pilot project, the investigators could recruit only a small sample and were primarily looking for postintervention improvement trends. Despite the sample size, the findings indicated that the effect size of the intervention was sufficient to contribute to significant improvements on a variety of measures.
A cohort of 18 women completed “Beyond MS” during 1996–1997 as part of an initial program evaluation funded by the Middle Tennessee Multiple Sclerosis Society. A second cohort of 19 women completed the same program in 2002–2003 as part of a pilot research project funded by the National Multiple Sclerosis Society. The two programs were led by the same group leader and the same coleader with MS, who served as both cofacilitator and role model. Both leaders were master’s-prepared psychiatric–mental health nurses with experience in group facilitation and group-based interventions. The group meetings were held from 6–8 pm on five consecutive Tuesdays. The 37 women all were high school graduates, as is not unusual among convenience samples of volunteers for educational interventions. Nineteen (51%) had college degrees, and 10 others had graduate degrees (27%). Twenty-five (68%) were married, eight were single, and four were divorced. Most were employed outside the home; 22 (60%) worked full time, and seven (19%) worked part time. Four (11%) were unemployed and on disability. Most listed their occupation as professional (51%), managerial (16%), or clerical (14%). One woman was African American; all of the others were White. The age range was 22–59 years (average and median age = 38 years). Thirteen (35%) had been diagnosed within the past year. The time since diagnosis ranged from a few weeks to 20 years; the average time was 5 years.
Procedure
This pilot study used a quasi-experimental design in which subjects acted as their own controls. Two preintervention measures were collected on each individual during a 5-week period. After meeting the entry criteria and giving written informed consent, participants completed and returned the first survey approximately 5 weeks before beginning the program (T1). Participants completed the same measures during the week before beginning the program (T2), immediately after completing the program (T3), and at a 6-month follow-up (T4). The T1 and T4 data were collected by mail. The T2 assessment was mailed to the participants before the program, completed at home before the participants reviewed any program material, and collected by the researchers at the first group session. The T3 assessment was completed at the end of the fifth group session to ensure timely postsession data collection. The two preintervention assessments (T1, T2) provided baseline data during a time period when there was no intervention, and the 6-month follow-up data (T4) allowed us to assess improvement, stabilization, or dissipation in the changes observed immediately after the intervention.
The researchers also collected open-ended feedback for program evaluation purposes. The participants completed a questionnaire about the program during the last group session and again at the 6-month follow-up.
Description of the Intervention Program
The format of the RA program was three group sessions accompanied by three videotapes and a manual. Because developing and using videotapes was not financially feasible in the MS study, the “Beyond MS” program was delivered in five group sessions and used only a manual. The manual contained readings and exercises designed to promote application of the content discussed in the group sessions. The topics covered in the sessions reflected the input of a focus group of women with MS who had evaluated the content of the original RA intervention program. In response to the focus group feedback, content was added related to coping with losses, uncertainty, depression, fatigue, and communication with health professionals.
Session 1. The first session addressed the mind-body connection and ways to set reasonable boundaries on the demands and expectations of others (e.g., supervisors, coworkers, family, friends). Women with MS deal with disease-related fatigue on a daily basis, and must learn to balance the needs of others with their own needs and limitations. Common reasons for difficulties with boundary setting were addressed. Women with MS must set effective boundaries to avoid undue stress and energy loss resulting from controlling or manipulative relationships or from failure to recognize their own boundaries with respect to others. Many individuals exert a great deal of energy trying to control people whom they cannot control.
Session 2. The discussion focused on the role of expectations, particularly negative or unrealistic expectations (e.g., perfectionism), in raising stress levels and how attributions about stressful events reflect a style of interpreting setbacks that can affect psychological distress and levels of optimism about the future. Common cognitive distortions also were discussed; these negative mental habits magnify stress by promoting anxious, pessimistic thought processes. The cognitive model for analyzing stressful situations was presented and applied (when requested) to specific situations presented to participants throughout the program.
Session 3. The topic was managing fears. Fatigue and pain management techniques were reviewed to enhance participants’ sense of control and self-efficacy. Cognitive reframing, a general stress management technique, was discussed and practiced.
Session 4. Constructive methods of anger and depression management were discussed, as were flexible problem solving and creative approaches to stressful circumstances.
Session 5. The discussion centered on ways to enhance social support, beginning with effective communication. Open, direct communication about boundaries, feelings, and the need for assistance and understanding can minimize stress in relationships. Common barriers to effective communication with healthcare providers were discussed. Finally, the facilitators provided practical information about dealing with insomnia.
At each session, the women were encouraged to identify content that could be applied to their lives and to set goals and practice changes in behavior related to the issues they identified. Although the “Beyond MS” program is broad in scope, a central theme is reinforced throughout the reading material, manual exercises, and group sessions: Individuals have some control over their response to an upsetting event or problem. This principle can be applied to any stressful situation. Altering one’s attitudes, expectations, and thought processes to be more positive, confident, relaxed, and realistic can alter the response to a situation. By letting go of the aspects of the problem beyond their control and aggressively dealing with their mental approach and the more malleable aspects of the problem, individuals can lessen their stress levels. Although the relationship between stress and MS exacerbation is still under investigation, more effective stress management skills should improve psychological outcomes, regardless of whether exacerbations can be prevented. Facilitators encouraged the participants to examine whether changes in attitudes, expectations, thought processes, or communication patterns could affect their stress levels and promote more adaptive coping behavior. The emphasis was on aggressively addressing malleable stressors and reactions to stress in general. The program’s positive tone is epitomized by the slogan “I have MS; it doesn’t have me.”
Measures
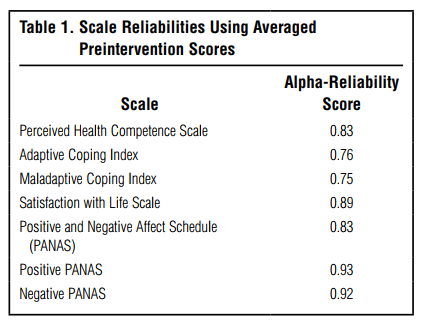
Data related to demographic and background variables (e.g., age, education, marital status, employment, race, length of time diagnosed with MS, medications) were collected at baseline. All of the following measures were completed by both cohorts at four different times, with the exception of the quality-of-life instrument, which was only used with the second cohort. All of these instruments have established validity and reliability, with extensive use in patient populations with chronic illness. The alpha reliability in this sample for all measures used in both cohorts is reported in Table 1.
Personal coping resources. The Perceived Health Competence Scale (Smith, Wallston, & Smith, 1995) is an 8-item measure of the extent to which individuals perceive control over their health status in general. Scores range from 1 to 5; higher scores indicate greater perceived control over health conditions.
Coping behavior. The 28-item brief COPE (Carver, 1997) was used to assess situational coping patterns. The participants were instructed to select the frequency with which they used coping strategies to deal with problems in their lives, particularly fatigue and MS-related problems. Scores range from 1 to 4, with higher scores indicating that participants use the coping strategies more frequently. The 13 subscales in this instrument that were derived from the original COPE instrument measure self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, religion, and acceptance.
Psychological well-being. The 5-item Satisfaction with Life Scale (Diener, Emmons, Larsen, & Griffin, 1985) was administered, along with the 20-item version of the Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988). Scores on the Satisfaction with Life Scale range from 1 to 6, with higher scores indicating greater life satisfaction. The PANAS contains two statistically independent, 10-item subscales assessing positive and negative affect. Participants were asked to record their feelings from the past week using the PANAS. Scores range from 1 to 5, with higher scores indicating greater frequency of a particular feeling noted within the past week. The negative-affect score from this instrument correlates highly with measures of depression (Smith, Wallston, & Dwyer, 1995).
Health-related quality of life. For the second cohort only, health-related quality of life was measured with an abbreviated version of the Multiple Sclerosis Quality of Life Instrument (MSQOL; Vickrey, Hays, Harooni, Myers, & Ellison, 1995). The MSQOL contains the SF-36 (Ware & Sherbourne, 1992) and adds 18 items to cover the domains of energy, health distress, pain, social function, sexual function and satisfaction, and overall quality of life. We substituted the SF-12 (Ware, Kosinski, & Keller, 1996) for the SF-36 to shorten the survey and lessen the burden on participants. The SF-12 provides reliable summary scores for both the Physical Component Summary and Mental Component Summary scales, reproducing at least 90% of the variance in the same summary scales using the SF-36. Score ranges vary by item on the SF-12, but higher scores indicate greater functionality on the measure. Each of the summary scales is composed of weighted-item contributions associated with eight subscales designed to measure functional health and well-being. These eight subscales assess general health, bodily pain, physical functioning, role limitations caused by physical problems, role limitations caused by emotional problems, social functioning, mental health, and vitality. As a construct, health-related quality of life incorporates outcomes for both physical well-being (reflected in the Physical Component Summary scale of the SF-12 and several subscales of the MSQOL), and psychological well-being (reflected in the Mental Component Summary scale of the SF-12 and several subscales of the MSQOL).
Physical well-being. All participants completed the 9-item Fatigue Severity Scale (Krupp, LaRocca, Muir-Nash, & Steinberg, 1989) to assess perceptions of fatigue intensity and its impact on their lives. Scores range between 1 and 7, with higher scores indicating greater fatigue levels.
Results
To test the first hypothesis (i.e., the postintervention scores will reflect a positive effect on patients’ perceptions of competence, coping behaviors, psychological well-being, healthrelated quality of life, and fatigue when compared to preintervention scores), the investigators used either t tests or multivariate analysis of variance (MANOVA) to compare pre- and postintervention mean scores. Multiple subscales or measures used with both cohorts were combined into appropriate indices for adaptive coping, maladaptive coping, and psychological well-being and used in within-subjects MANOVAs over four points in time, with subsequent univariate analyses of individual measures used when indicated.
An index of personal coping resources could not be constructed, because only one measure for this construct was used in both cohorts—perceived health competence. Comparison of averaged preintervention scores with averaged postintervention scores revealed that the perceived health competence mean of 3.41 (SD = 0.62) rose to 3.67 (SD = 0.69). This change indicated a significant improvement in perceived competence (t [33] = 3.16; p < .01). The effect size for this variable was 0.23.
The Brief COPE contains 13 subscales that were derived from a longer version of the COPE, which was used with the earlier cohort. From a theoretical perspective, four of these subscales could be classified as maladaptive in this patient population—venting, denial, self-distraction, and behavioral disengagement. The other candidate for consideration in this index was substance abuse, but the wording of the items did not differentiate between use of alcohol and the use of prescription medications, which is useful and adaptive in this patient population. Therefore, the substance abuse subscale was not included in the Maladaptive Coping Index. The MANOVA results for the Maladaptive Coping Index were significant (F [3, 29] = 3.85; p = .02), justifying exploration of univariate measures used in this index. Planned comparisons of averaged preintervention with averaged postintervention scores revealed significant decreases in two maladaptive subscales: self-distraction (t [34] = -2.40; p < .03) and venting (t [34] = -2.26; p < .04). Table 2 displays the pre- and postintervention means of the Maladaptive Coping subscales and the results of univariate analysis of these subscales.
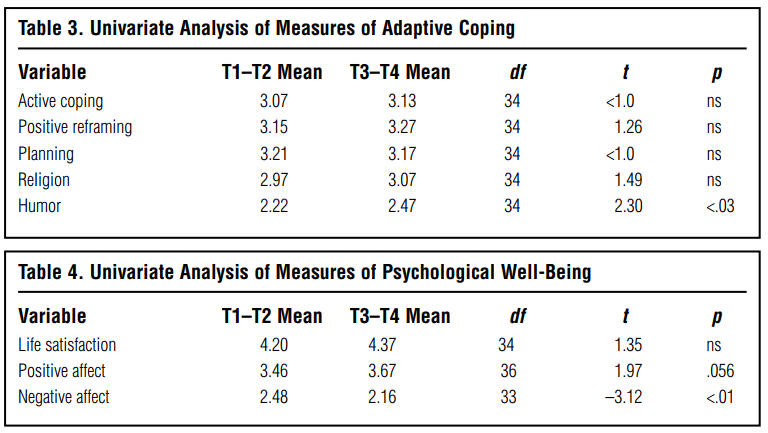
A separate Adaptive Coping Index was constructed from five theoretically adaptive subscales—active coping, positive reframing, planning, use of religion, and use of humor. Other subscale candidates for this index could be viewed as either adaptive or maladaptive and therefore were omitted. These subscales included acceptance, which could be adaptive or associated with passivity, as well as use of emotional support and use of instrumental support, which could be adaptive or associated with excessive dependence. The MANOVA results for the Adaptive Coping Index were significant (F [3, 32] = 4.08; p < .02), justifying exploration of univariate measures used in this index. The subscale related to use of humor reflected significant improvement (t [34] = 2.3; p < .03). Table 3 displays the pre- and postintervention means of the adaptive coping subscales and the results of univariate analysis of these subscales.
To measure psychological well-being outcomes, a Psychological Well-Being Index was created from the Satisfaction with Life Scale positive and negative subscales of the PANAS. These three measures of psychological well-being were combined into a Psychological WellBeing Index for the purposes of multivariate analysis. The MANOVA was significant (F [9, 222] = 2.30; p < .02). Univariate analysis of the individual measures of psychological well-being could therefore be explored. Using planned comparisons of averaged preintervention scores with averaged post intervention scores, the negative affect subscale of the PANAS reflected significant improvement (t [33] = –3.12; p < .01). The effect size for this variable was 0.24. Improvements in the positive affect subscale of the PANAS were nearly significant (t [33] = 1.97; p < .06). There were no significant changes in life satisfaction scores, although there was a trend toward greater life satisfaction. Table 4 displays the preand postintervention means for the three measures of psychological well-being and the results of univariate analysis of these measures.
The MSQOL instrument was completed only by the second cohort (n = 19). Significant improvements were evident in this small sample. Averaged preintervention scores were compared with averaged postintervention scores, and the standard SF-12 algorithm was then used to compute the 8 subscales and 2 summary scales. There were no significant changes in the Physical Component Summary scale, but the Mental Component Summary scale (MCS-12) was significantly improved from a preintervention mean of 42 to a postintervention mean of 47 (t [17] = 2.32; p = .03). Although the SF-12 does not provide for reliable interpretation of changes in the 8 individual subscales, the summary scale interpretations are highly reliable and the MCS-12 summary scale is highly correlated with three subscales—mental health, social functioning, and role limitations stemming from emotional problems (Ware, Kosinski, & Keller, 1996).
The MSQOL provides additional items related to health-related quality of life. Some of these scales also demonstrated significant improvement, despite the small sample size. Scores on the health-distress subscale reflected significant improvement (t [17] = –5.09; p < .001), as did the satisfaction with sexual function subscale (t [16] = 2.14; p < .05).
Other than the Physical Component Summary score from the SF-12, the only measure of physical outcomes used was the Fatigue Severity Scale. There were no significant improvements in fatigue severity scores, although the trend was in a positive direction, with the preintervention mean of 5.67 decreasing to a post intervention mean of 5.59.
With respect to the first hypothesis, significant postintervention improvements were noted in perceived competence, adaptive and maladaptive coping indices, psychological well-being, and health-related quality-oflife scores. There were no significant improvements in physical outcomes. The first hypothesis was basically supported in this pilot sample.
With respect to the second hypothesis (i.e., compared to initial postintervention scores, 6-month follow-up scores will reflect stabilization or improvement), comparisons between initial postintervention scores and 6-month followup scores on perceived health competence, coping behaviors, psychological well-being, health-related quality of life, and fatigue did stabilize or improve. The second hypothesis was therefore supported. The one significant change, in the Maladaptive Coping Index, reflected continued improvement over the follow-up period (t [33] = –2.44; p = .02), primarily because of a continuation of decreases in scores on the venting and behavioral disengagement coping subscales.
Preliminary Qualitative Analysis
To help us collect open-ended feedback for program evaluation purposes, the participants filled out a questionnaire about the program during the last group session and at 6-month follow-up. There were four questions.
“Which aspects of the program were most helpful to you?” There were four major categories of responses. The women stated that they (a) enjoyed being with other women who shared their concerns, fears, and frustrations and who could relate to their feelings; (b) enjoyed the type of social interaction the group promoted, particularly camaraderie and laughter; (c) learned a great deal from the program material and one another about managing stress and symptoms (because of the sharing of ideas and experience); and (d) gained hope for living a more normal life with MS.
“Have you made any changes in your approach to challenges because of anything learned in the program?” Participants offered a wider spectrum of responses, as well as more specific responses. Their replies reflected nine types of changes: (a) they noted a more realistic acknowledgement and acceptance of their limitations; (b) they challenged unrealistic, perfectionistic expectations of themselves and thus were able to be more tolerant of themselves; (c) they set healthy boundaries on others who had unrealistic expectations of them; (d) they became more assertive in asking for help; (e) they tried to challenge negative, self-destructive thinking patterns; (f) they absorbed new tools for managing challenges (specifically, reframing); (g) they began to face their challenges with a more positive, optimistic attitude; (h) they noted more creativity in their approach to problem solving; and (i) they noted positive changes in friendships because of heightened tolerance and interpersonal sensitivity. One participant offered a concise summary of her new attitude toward her unpredictable disease: “I have MS. I can’t really do anything about that. I am still a person who can contribute to society, and I just need to seek out my role and carry through with it. When the MS prevents me from doing what I want, so what? I may have to rest more during certain times, but that is OK, too.”
“Do you have any suggestions for changes in the program (either content or format)?” Several women would have preferred a longer program (i.e., more sessions). Some suggested that the manual and questionnaires be made available online for greater convenience. Some suggested that more time be devoted to discussion of homework questions. Comments regarding the manual were universally positive. The group members agreed that the 2-hour session time was appropriate. (Longer sessions would have been too tiring, particularly because they took place after many participants’ work day.)
“How satisfied were you with the program?” No one indicated dissatisfaction with the program in any way.
Discussion
The intervention was based on the Lazarus and Folkman Stress and Coping Model (1984), which underscores the pivotal role of perceptions in adaptation to stress. This model suggests that an intervention designed to enhance a sense of competence would positively affect appraisals of stressors, thereby affecting coping patterns and psychological outcomes. Consistent with the Lazarus and Folkman theory, our intervention apparently affected perceived health competence, coping behaviors, and subsequent psychological outcomes. A larger sample would enable exploration of path analysis to determine whether the direction of impact among the variables was also consistent with the theory.
The intervention affected psychological outcomes in a positive manner. The improvement in the healthdistress subscale scores of the MSQOL was consistent with the change noted in the negative affect subscale of the PANAS. In addition, the positive affect subscale of the PANAS registered nearly significant improvement (p < .06). These findings were consistent with the significant improvements related to the Mental Component Summary scale of the SF-12, which reflects psychological well-being. This summary scale correlates highly with the three subscales related to mental health, social functioning, and role limitations stemming from emotional problems (Ware et al., 1996). The findings related to our measures of psychological well-being, including subscales from the health-related quality-of-life measure, were therefore consistent and theoretically predictable. The Satisfaction with Life Scale was the only measure related to psychological well-being that did not reflect improved scores, although there was a trend in a positive direction. The Satisfaction with Life Scale contains 5 items, including In most ways my life is ideal; If I could live my life over, I would change almost nothing; and The conditions of my life are excellent. It is hard to imagine that a woman with MS would endorse these items in an extremely positive way. It is therefore not surprising that no changes were noted in the scores from this instrument.
It is very difficult to positively affect physical outcomes when dealing with a progressive disease such as MS, so changes in reported fatigue severity were not expected. For the same reason, we were not surprised by the lack of improvement in the Physical Component Summary scale of the SF-12, which is focused on physical functionality. (Additional factors are that the intervention may have been too brief to elicit positive changes in fatigue levels and that it did not have an exercise component.)
This pilot study had limitations related to the small sample size and relative homogeneity of the sample. The program needs further testing among both women and men who are in different stages of MS, as well as among members of different demographic groups, specifically less well-educated and more ethnically diverse participants. Circumstances did not allow us to use randomized wait-list control groups in this study. On a positive note, the intervention is theoretically based, it elicited a similar pattern of significant improvements in a sample of women with RA, and it demonstrated significant improvements despite the small sample size.
The “Beyond MS” program resulted in significant improvements in perceived health competence, coping behaviors, and a variety of psychological outcomes in a relatively small sample. Furthermore, the program was cost effective, using a manual and five group sessions to deliver its outcomes. The “Beyond MS” program is positive in tone; it encourages aggressive action when change is possible and acceptance of the unchangeable. The group dynamic was positive. Participants felt free to express feelings, embracing the type of sharing and empathy that can readily develop among individuals who face similar challenges. There is a great need for a positive program to promote adaptive coping in the MS population, and we believe “Beyond MS” has demonstrated its potential for effective use. The optimal psychosocial intervention program for individuals with MS, in terms of effectiveness and efficiency of delivery, might include features from several interventions discussed in the literature. Future studies are needed to explore aspects of effective psychosocial interventions and their effect on various types of participants, so that interventions can be matched to the individuals most likely to benefit from them. The “Beyond MS” program was well received by our participants, and the findings warrant further investigation into its usefulness.
Acknowledgments
The authors gratefully acknowledge their funding sources. The initial program evaluation was supported by the Middle Tennessee Multiple Sclerosis Society and the Iota Chapter of Sigma Theta Tau Honorary Nursing Society. The pilot research study was funded by the National Multiple Sclerosis Society. The authors gratefully acknowledge Joseph Hepworth, PhD, for his statistical consultation on this project.
References
Ackerman, K. D., Heyman, R., Rabin, B. S., Anderson, B. P., Houck, P. R., Frank, I., et al. (2002). Stressful life events precede exacerbations of multiple sclerosis. Psychosomatic Medicine, 64, 916–920.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (1998). Health promotion from the perspective of social cognitive theory. Psychology and Health, 13, 623–649.
Beatty, W. W. (1993). Cognitive and emotional disturbances in multiple sclerosis. Neurologic Clinics, 11, 189–204.
Brassington, J. C., & Marsh, N. V. (1998). Neuropsychological aspects of multiple sclerosis. Neuropsychology Review, 8, 43–77.
Buelow, J. M. (1991). A correlational study of disabilities, stressors and coping methods in victims of multiple sclerosis. Journal of Neuroscience Nursing, 23, 247–251.
Buljevac, D., Hop, W. C., Reedeker, W., Janssens, A. C., van der Meche, F. G., va Doorn, P. A., et al. (2003). Self-reported stressful life events and exacerbations in multiple sclerosis: Prospective study. British Medical Journal, 327, 646.
Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the Brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100.
Chwastiak, L., Ehde, D. M., Gibbons, L. E., Sullivan, M., Bowen, J. D., & Kraft, G. H. (2002). Depressive symptoms and severity of illness in multiple sclerosis: Epidemiologic study of a large community sample. American Journal of Psychiatry, 159, 1862–1868.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Erlbaum.
Crawford, J. D., & McIvor, G. P. (1985). Group psychotherapy: Benefits in multiple sclerosis. Archives of Physical Medicine and Rehabilitation, 66, 810–813.
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75.
Foley, F. W., & Bedell, J. R. (1987). Efficacy of stress-inoculation training in coping with multiple sclerosis. Journal of Consulting and Clinical Psychology, 6, 919–922.
Frohman, E. M. (2003). Multiple sclerosis. Medical Clinics of North America, 87, 867–897.
Ferreras, J., Junquera, L. M., & Garcia-Consuegra, L. (2000). Intracranial placement of a nasogastric tube after severe craniofacial trauma. Oral Surgery, Oral Medicine, and Oral Pathology, 90(5), 564–566.
Giraudet-Le Quintrec., J. S., Coste, J., Vastel, L., Pacault, V., Jeanne, L., Lamas, J. P., et al. (2003). Positive effect of patient education for hip surgery. Clinical Orthopaedics and Related Research, 414, 112–120.
Gozur, J. A. (1987). Postoperative tension pneumocephalus. Journal of Neuroscience Nursing, 19(1), 30–35.
Iplikcioglu, A. C., Bek, S., Bekmaz, K., & Basocak, K. (2003). Tension pneumocyst after transsphenoidal surgery for Rathke’s cleft cyst. Neurosurgery, 52(4), 960–962.
Gulick, E. E. (2001). Emotional distress and activities of daily living functioning in persons with multiple sclerosis. Nursing Research, 50, 147–154.
Hainsworth, M. A. (1994). Living with multiple sclerosis: The experience of chronic sorrow. Journal of Neuroscience Nursing, 26, 237–240.
Hartings, M. F., Pavlou, M. M., & Davis, F. A. (1976). Group counseling of MS patients in a program of comprehensive care. Journal of Chronic Diseases, 29, 65–73.
Holland, N. J. (2004). Clinical bulletin: Information for health professionals. New York: National Multiple Sclerosis Society.
Kroencke, D. C., Denney, D. R., & Lynch, S. G. (2001). Depression during exacerbations in multiple sclerosis: The importance of uncertainty. Multiple Sclerosis, 7, 237–242.
Krupp, L. B., LaRocca, N. G., Muir-Nash, J., & Steinberg, A. D. (1989). The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Archives of Neurology, 46, 1121–1123.
Kurtzke, J. F. (1983). Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology, 33, 1444–1452.
Larcombe, N. A., & Wilson, P. H. (1984). An evaluation of cognitivebehavior therapy for depression in patients with multiple sclerosis. British Journal of Psychiatry, 145, 366–371.
Laviola, S., Kirvela, M., Spoto, M. R., Tschuor, S., & Alon, E. (1999). Pneumocephalus with intense headache and unilateral papillary dilation after accidental dural puncture during epidural anesthesia for cesarean section. Anesthesie et Analgesie, 88(3), 582–583.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer.
Levine, H. (1991). Endoscopic diagnosis and management of CSF rhinorrhea. Operative Techniques in Otolaryngology Head Neck Surgery, 2(4), 282–284.
Mathiowetz, V., Matuska, K. M., & Murphy, M. E. (2001). Efficacy of an energy conservation course for persons with multiple sclerosis. Archives of Physical Medicine and Rehabilitation, 82, 449–456.
McGuinness, S. (1996). Learned helplessness in the multiple sclerosis population. Journal of Neuroscience Nursing, 28, 163–170.
Minden, S. L. (1992). Psychotherapy for people with multiple sclerosis. Journal of Neuropsychiatry and Clinical Neurosciences, 4(2), 198–213.
Mohr, D. C., & Cox, D. (2001). Multiple sclerosis: Empirical literature for the clinical health psychologist. Journal of Clinical Psychology, 57, 479–499.
Mohr, D. C., Goodkin, D. E., Nelson, S., Cox, D., & Weiner, M. (2002). Moderating effects of coping on the relationship between stress and the development of new brain lesions in multiple sclerosis. Psychosomatic Medicine, 64, 803–809.
Mohr, D. C., Hart, S. L., Julian, L., Cox, D., & Pelletier, D. (2004). Association between stressful life events and exacerbation in multiple sclerosis: A meta-analysis. British Medical Journal, 328, 731–741.
Mohr, D. C., Likosky, W., Bertagnolli, A., Goodkin, D. E., Wende, J. V., Dwyer, P., et al. (2000). Telephone-administered cognitivebehavioral therapy for the treatment of depressive symptoms in multiple sclerosis. Journal of Consulting and Clinical Psychology, 68, 356–361.
Murray, T. J. (1995). The psychosocial aspects of multiple sclerosis. Neurologic Clinics, 13, 197–221.
Pavlou, M., Hartings, M., & Davis, F. A. (1978). Discussion groups for medical patients. Psychotherapy and Psychosomatics, 30, 105–115.
Schiffer, R. B. (1990). Disturbances of affect. In S.M. Rao (Ed.), Neurobehavioral aspects of multiple sclerosis. New York: Oxford University Press.
Schwartz, C. E. (1999). Teaching coping skills enhances quality of life more than peer support: Results of a randomized trial with multiple sclerosis patients. Health Psychology, 18, 211–220.
Schwartz, C. E., Coulthard-Morris, L.,& Zeng, Q. (1996). Psychosocial correlates of fatigue in multiple sclerosis. Archives of Physical Medicine and Rehabilitation, 77(2), 165–170.
Schwartz, C. E., & Rogers, M. (1994). Designing a psychosocial intervention to teach coping flexibility. Rehabilitation Psychology, 39, 61–76.
Schrijver, H. M., & Berendse, H. W. (2003). Pneumocephalus by Valsalva maneuver. Neurology, 60(2), 345–346.
Scott, A. (2004). Managing anxiety in ICU patients: The role of pre-operative information provision. Nursing in Critical Care, 9(2), 72–79.
Sinclair, V. G., Wallston, K. A., Dwyer, K. A., Blackburn, D. S., & Fuchs, H. (1998). Effects of a cognitive-behavioral intervention for women with rheumatoid arthritis. Research in Nursing & Health, 21, 315–326.
Smith, C. A., Wallston, K. A., & Dwyer, K. A. (1995). On babies and bathwater: Disease impact and negative affectivity in the selfreports of persons with rheumatoid arthritis. Health Psychology, 14, 64–73. Head and Neck Surgery, 111, 600–605.
Smith, M. S., Wallston, K. A., & Smith, C. A. (1995). The development and validation of the Perceived Health Competence Scale. Health Education Research: Theory and Practice, 10, 51–64.
Spiegelberg, N. (1980). Support group improves quality of life. Rehabilitation Nursing, 5, 9–11.
Sprague, A., & Poulgrain, P. (1999). Tension pneumocephalus: A case report and literature review. Journal of Clinical Neuroscience, 6(5), 418–424.
Stankiewicz, J. (1991). CSF fistula and endoscopic sinus surgery. Laryngoscope, 101(Mar), 250–256.
Suri, A., Mahapatra, A. K., & Singh, V. P. (2000). Posterior fossa tension pneumocephalus. Child’s Nervous System, 16(4), 196–199.
Stuifbergen, A. K., & Becker, H. (1994). Predictors of health promoting lifestyles in persons with disabilities. Research in Nursing and Health, 17, 3–13.
Stuifbergen, A. K., Becker, H., Blozis, S., Timmerman, G., & Kullberg, V. (2003). A randomized clinical trial of a wellness intervention for women with multiple sclerosis. Archives of Physical Medicine and Rehabilitation, 84, 467–476.
Stuifbergen, A. K., Seraphine, A., & Roberts, G. (2000). An explanatory model of health promotion and quality of life in chronic disabling conditions. Nursing Research, 49(3), 122–129.
Uemura, K., Meguro, K., & Matsumura, A. (1997). Pneumocephalus associated with fracture of thoracic spine. British Journal of Neurosurgery, 11(3), 253–256.
Van der Werf, S. P., Evers, A., Jongen, P. J., & Bleijenberg, G. (2003). The role of helplessness as mediator between neurological disability, emotional instability, experienced fatigue and depression in patients with multiple sclerosis. Multiple Sclerosis, 9(1), 89–94.
Van Heerden, P. V., Pinder, M., & Cameron, P. D. (1999). Pneumocephalus and resuscitation. Anesthesia and Intensive Care, 27(2), 223–224.
Vickrey, B. G., Hays, R. D., Harooni, R., Myers, L. W., & Ellison, G. W. (1995). A health-related quality of life measure for multiple sclerosis. Quality of Life Research, 4, 187–206.
Wanamaker, J. R., Mehle, M. E., Wood, B. G., & Lavertu, P. (1995). Tension pneumocephalus following craniofacial resection. Head and Neck, 17(2), 152–156.
Ware, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary test of reliability and validity. Medical Care, 34, 220–233.
Ware, J. E., & Sherbourne, C. D. (1992). A 36-item short-form health survey (SF-36): Conceptual framework and item selection. Medical Care, 30, 473–483.
Wassem, R. (1991). A test of the relationship between health locus of control and the course of multiple sclerosis. Rehabilitation Nursing, 16, 189–193.
Wassem, R. (1992). Self-efficacy as a predictor of adjustment to multiple sclerosis. Journal of Neuroscience Nursing, 24, 224–229.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070.
Wein, F. B., & Gans, M. S. (1999). The perils of a sneeze. Journal of Neuro-ophthalmology, 19(2), 128–130.
Wineman, N. M., Durand, E. J., & Steiner, R. P. (1994). A comparative analysis of coping behaviors in persons with multiple sclerosis or a spinal cord injury. Research in Nursing & Health, 17, 185–194.
Wineman, N. M., Schwetz, K. M., Goodkin, D. E., & Rudick, R. A. (1996). Relationships among illness uncertainty, stress, coping, and emotional well-being at entry into a clinical drug trial. Applied Nursing Research, 9(2), 53–60.
Wood, B. J., Mirvis, S. E., & Shanmuganathan, K. (1996). Tension pneumocephalus and tension orbital emphysema following blunt trauma. Annals of Emergency Medicine, 28(4), 446–449.
Yates, H., Hamill, M., Borel, C. O., & Toung, T. J. (1994). Incidence and perioperative management of tension pneumocephalus following craniofacial resection. Journal of Neurosurgical Anesthesiology, 6(1), 15–20.
Zasler, N. D. (1999). Posttraumatic tension pneumocephalus. The Journal of Head Trauma Rehabilitation, 14(1), 81–84.