MRI monitoring of spinal cord changes

Selected By
Lori Mayer, DNP, MSN, RN, MSCN
Why is this important to me?
Healthcare providers use magnetic resonance imaging (MRI) of the brain to help them diagnose MS as well as to watch changes in the brain both as the disease progresses and to see how individuals respond to therapy. However, MS affects not only the brain, but also the spinal cord. Symptoms of spinal cord involvement may include problems with muscle movement and sensory problems such as numbness. Thus, healthcare professionals also use MRI to watch for changes in the spinal cord. MRI of the spinal cord is more challenging than MRI of the brain in part because the spinal cord is a small structure, and breathing and blood vessel pulsation can affect the image.
What is the objective of this study?
The authors reviewed the advantages and challenges associated with MRI for monitoring changes in the spinal cord.
Conventional MRI is a valuable imaging tool because of its ability to detect lesions in the spinal cord. MRI shows spinal cord lesions in about 90% of people who have MS. Spinal cord lesions are more common in areas close to the neck compared to areas close to the tail bone.
MRI of the spinal cord can be performed with different settings of the scanner, allowing:
- Precise views of lesions
- Detection of shrinkage of the spinal cord, which is associated with disability
The number and type of lesions in the spinal cord that MRI may show differ depending on the type of MS. People who have
- Clinically isolated syndrome (CIS)typically have fewer lesions on their spinal cords. When individuals who have been diagnosed with CIS have multiple spinal cord lesions, they may experience more severe symptoms.
- Relapsing-remitting MS usually have many spinal cord lesions.
- Secondary progressive MS often have many spinal cord lesions accompanied by shrinkage of the spinal cord.
- Primary progressive MS usually have more lesions on their spinal cord than on their brain.
- Progressive MS typically have mild abnormalities along the length of the spinal cord.
The presence and the type of abnormalities found on spinal cord MRI early during the disease provides valuable information about diagnosis and prognosis. Among the reasons that a healthcare professional may request a spinal cord MRI include:
- For individuals who are not experiencing symptoms and whose brain MRI reveals lesions, a spinal cord MRI may help their healthcare provider predict whether they will develop CIS or primary progressive MS.
- For people who have spinal cord symptoms (muscle problems, numbness, tingling, etc.), spinal cord MRI can help to confirm a diagnosis of MS.
- If your brain MRI results are inconclusive or if you have unusual spinal cord symptoms, a spinal cord MRI may help with diagnosis.
- Addition of spinal cord MRI to brain MRI for routine clinical monitoring of an individual’s MS may identify disease activity that may not otherwise be detected. This enables a healthcare professional to provide earlier treatment that may be more effective.
Research scientists are actively exploring new ways to improve spinal cord MRI techniques. Although advanced and quantitative spinal cord MRI techniques are not part of routine clinical use, they may someday improve management of MS by:
- Predicting spinal cord shrinkage earlier. Shrinkage is present in the upper spinal cord very early in MS. Shrinkage rates are higher in the spinal cord than in the brain, especially among patients who have secondary progressive MS. Shrinkage is also higher in patients with worsening disease compared to those with stable disease.
- Seeing microscopic types of damage characteristic of MS, which are not seen in CIS. These microscopic types of damage are more pronounced in people with higher levels of disability. Newer MRI methods show greater sensitivity for detecting these changes than conventional MRI.
- Seeing lesions associated specifically with sensory and muscle impairment and disability.
- Understanding the differences in the ways in which people who have MS and those who do not perform certain tasks.
- Detecting recovery from symptoms and repair of damage.
- Assessing disability in people who have had MS for a long time.
How did the authors study this issue?
The authors reviewed different methods of performing spinal cord MRI and what can be observed with spinal cord MRI in people with MS and related diseases.
| SHARE: | |||||
Original Article
MRI monitoring of spinal cord changes in patients with multiple sclerosis
Current Opinion in Neurology
Rovira, Alex; de Stefano, Nicola
ABSTRACT
Purpose of review
We analyze recent data on technical aspects, clinical indications, and imaging features of spinal cord MRI in multiple sclerosis, and on the value of this examination for assessing the type and extension of spinal cord damage, and for predicting prognosis in patients with this disease.
Recent findings
Spinal cord MRI on patients with multiple sclerosis is technically challenging and a standardized protocol that optimizes the accuracy of this examination is essential, particularly as recent studies have shown its value for diagnostic and prognostic purposes. Several recent studies have proven the potential value of new, quantitative spinal cord magnetic resonance metrics for assessing the type and degree of spinal cord damage. Although these measures can bring new insights into the understanding of the disease, there is not enough evidence to support their use outside the research scenario.
Summary
Neurologists and neuroradiologists should be aware of the added value of conventional spinal cord MRI in the initial diagnosis and monitoring of multiple sclerosis. The use of advanced quantitative magnetic resonance techniques, which better assess the degree of irreversible tissue damage within the spinal cord, is mainly restricted to clinical research and cannot yet be incorporated into the daily clinical practice.
INTRODUCTION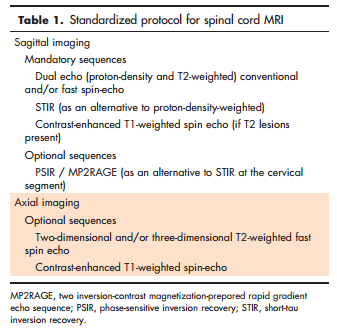
In this review, we will discuss the technical aspects and some improvements of spinal cord MRI, the typical MRI features of the spinal cord in multiple sclerosis, and the clinical indications for this examination. Finally, we will analyze recent data on the value of different quantitative magnetic resonance techniques for assessing the type and degree of spinal cord damage, which is particularly relevant in the progressive phases of the disease in which spinal cord MRI is increasingly used as a biomarker of disease progression.
SPINAL CORD MAGNETIC RESONANCE IMAGING: TECHNICAL FEATURES MRI of the spinal cord is more challenging than imaging of the brain in patients with multiple sclerosis. The spinal cord is a small, mobile structure and acquisition of high-quality images is challenging. The evaluation is further complicated by the common presence of ghosting [breathing, vessel and cerebrospinal fluid (CSF) pulsations] and truncation artifacts [1,2], which can lead to falsenegative and false-positive interpretations. Several technical improvements minimize these difficulties, such as spatial presaturation slabs and fast imaging sequences, which, in combination with spinal phased-array coils, allow rapid imaging of the whole spinal cord within clinically acceptable acquisition times. Selection of an appropriate T2-weighted sequence is essential to obtain diagnostic images. For sagittal imaging, conventional or fast dual-echo (proton density and T2-weighted, acquired in combination or independently) spin-echo sequences should be considered the reference standard. Adequate selection of the first echo time is crucial to render the spinal cord isointense to CSF, as this facilitates identification of increases in signal intensity within the spinal cord [2] and is particularly relevant for depicting diffuse lesions. Short-tau inversion recovery (STIR) T2-weighted sequences seem to increase the sensitivity of conventional or fast T2-weighted sequences, by improving the lesion/cord contrast-to-noise ratio [3]. However, this sequence is more susceptible to flow-related artifacts, has lower image quality and lower interobserver agreement, and is more time-consuming than conventional/fast T2-weighted sequences. Therefore, STIR should be considered as a complementary sequence (to T2-weighted sequences) in the detection of spinal cord multiple sclerosis lesions, but cannot be used in isolation because of its low specificity [4] (Table 1). A recent preliminary study has shown that three-dimensional double inversion recovery (DIR) sequences, which have shown to increase the sensitivity of brain MRI in depicting cortical and infratentorial lesions, also improves the detection of multiple sclerosis lesions in the spinal cord compared to conventional two-dimensional T2-weighted sequences [5]. Finally, it has been shown that heavily T1-weighted sequences, such as phase-sensitive inversion recovery (PSIR) or two inversion-contrast magnetization-prepared rapid gradient echo (MP2RAGE), improve multiple sclerosis lesion detection, not only in the brain, but also in the cervical spinal cord [6,7]. The three-dimensional acquisition of these sequences allows the generation of multiplanar reconstructions, and a more precise delineation of lesions (Fig. 1).
Spinal cord grey matter imaging cannot be obtained with conventional MRI techniques because of their limited spatial resolution and contrast between grey matter and white matter. This limitation has been partially overcome with the introduction of high-resolution axial PSIR sequences, which in a relatively short acquisition time can provide spinal cord imaging of grey matter. These images can be used to detect grey matter atrophy invivo, which contributes more to patient disability than global spinal cord or brain atrophy [8].
CONVENTIONAL SPINAL CORD MRI FEATURES
Focal or diffuse spinal cord signal abnormalities on T2-weighted MRI resembling those seen in the brain are detected in up to 90% of patients with a clinical diagnosis of multiple sclerosis [9]. These lesions involve the cervical region more often than the thoracic or lumbar regions [10], and in sagittal views they characteristically have a ‘cigar’ shape and rarely exceed two vertebral segments in length. On crosssection they typically occupy the lateral and posterior white matter columns and do not spare the central grey matter. The lesions rarely affect the anterior columns or central cord area and seldom occupy more than half the cross-sectional area of the cord [10,11& ]. This is usually different from what is seen in neuromyelitis optica (NMO), where cord lesions typically extend over three or more contiguous vertebral segments and occasionally the entire spinal cord (longitudinally extensive spinal cord lesions), are centrally located (preferential centra grey matter involvement) and affect much of the cross-section on axial images [12& ].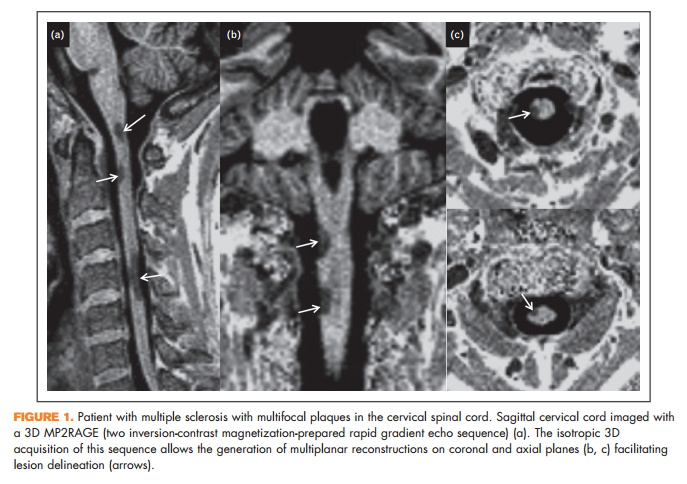
In some patients, mainly those with a progressive multiple sclerosis disease course, diffuse mild signal abnormalities, better identified on protondensity weighted and STIR sequences, [1,13& ] predominate along extensive segments of the spinal cord, and sometimes they are the only finding.
The prevalence and type of spinal cord lesions differ according to the clinical multiple sclerosis phenotype. Relapsing remitting multiple sclerosis typically shows multiple focal lesions, whereas in secondary progressive multiple sclerosis, the abnormalities are more extensive and diffuse and are commonly associated with spinal cord atrophy [14]. In primary progressive multiple sclerosis, the cord abnormalities are quite extensive in comparison with the brain abnormalities. This discrepancy may help to diagnose primary progressive multiple sclerosis in patients with few or no brain abnormalities. In patients with a clinically isolated syndrome (CIS), the prevalence of spinal cord lesions is lower, particularly if there are no spinal cord symptoms. Nevertheless, asymptomatic cord lesions are found in 30–40% of patients with a nonspinal cord CIS, a prevalence that is similar in patients with a radiologically isolated syndrome (RIS) [15–17].
Enhancing multiple sclerosis lesions are seen less frequently in the spinal cord than in the brain (new enhancing lesions are four to ten times more common in brain than cord), but are commonly associated with new clinical symptoms and with concomitant enhancing brain lesions [18,19]. Several factors may explain this lower prevalence, such as the lower volume of the spinal cord compared to the brain, and lower enhancing conspicuity as a result of a less optimal imaging technique, poor tissue contrast, and interfering flow artifacts, or because of more frequent use of high-dose corticosteroids for spinal cord symptoms, which can mask enhancement [20]. Use of a high gadolinium dose and long postinjection delay may increase the sensitivity for detecting these enhancing lesions [21].
SPINAL CORD MRI FOR THE DIAGNOSIS AND PROGNOSIS OF MULTIPLE SCLEROSIS 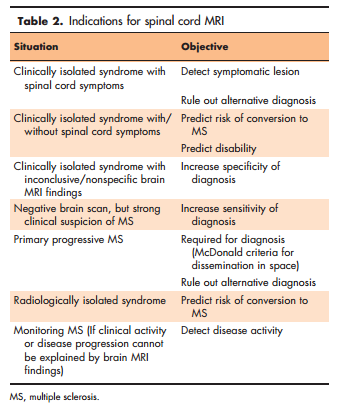
Indications for spinal cord MRI vary depending on the clinical situation and the brain findings [13& ] (Table 2). To establish the diagnosis, spinal cord MRI is mandatory in patients with spinal cord symptoms at disease onset, mainly to exclude treatable lesions such as extrinsic compression, neoplasm, or vascular malformation [15]. In addition, the examination is helpful when brain MRI results are inconclusive; that is, when diagnostic criteria for dissemination in space are not met, but the lesion(s) are typical of magnetic resonance [15]. In this latter situation, adding spinal cord to brain MRI could be of clinical relevance, as detection of spinal cord lesions might facilitate the diagnosis of multiple sclerosis and is predictive of conversion to clinically definite multiple sclerosis (CDMS) [1]. Similarly, diagnostic certainty can be increased in patients with nonspecific brain MRI findings, because asymptomatic cord lesions are relatively common in multiple sclerosis, but are rare in other white matter diseases (cerebrovascular or other autoimmune inflammatory disorders, aging-related or migraine-related focal white matter abnormalities) [22,23]. In addition, the presence of asymptomatic spinal cord lesions in patients with brain MRI findings suggesting an RIS heralds an increased risk of progression to a CIS or to primary progressive multiple sclerosis in a short time, regardless of the brain imaging findings [16].
It would be expected that the presence of spinal cord lesions could predict the functional outcome of patients with early multiple sclerosis, as it has been shown for infratentorial lesions [24]. A study performed in patients with CIS presenting with a spinal cord syndrome has shown that a high number of cord lesions at baseline predict a poorer clinical outcome [25]. It has been also shown that asymptomatic spinal cord lesions, even in patients with optic neuritis, predict not only the time to development of clinically definite multiple sclerosis, but also the degree of future disability [14]. Finally, Coret et al. [26] reported that not only the presence but also the pattern of spinal cord magnetic resonance lesions might be valuable, as early relapsingremitting patients with multiple sclerosis with a diffuse lesion pattern reached a high degree of clinical disability sooner than those without. All these data indicate that presence and type of spinal cord magnetic resonance abnormalities early in the disease course provide valuable prognostic information, and recommend the acquisition of spinal cord MRI at initial multiple sclerosis diagnosis [24,27–29].
CONTRIBUTION OF CONVENTIONAL SPINAL CORD MRI FOR MONITORING MULTIPLE SCLEROSIS
Different studies have demonstrated that the presence of new asymptomatic lesions (T2 and enhancing T1) on brain MRI scans predict recurrence of relapses, supporting the use of this simple metrics as clinical surrogates both in clinical trials and in clinical practice [30]. However, spinal cord is not commonly used for this purpose for several reasons: the frequency of new cord lesions is considerably lower than that of new brain lesions; there is a relationship between development of new lesions in the brain and development of new lesions in the spinal cord (although may occur independently of new brain lesions) [9]; and incorporating spinal cord MRI in routine monitoring of the disease significantly increases the acquisition time [18,31,32]. Despite these limitations, spinal cord MRI is usually performed for multiple sclerosis monitoring in clinical practice, when patients present atypical or unexpected new spinal cord symptoms or when clinical activity or disease progression cannot be explained by brain MRI findings.
Recently, a study has addressed the independent value of spinal cord MRI in monitoring disease evolution. This has shown that adding spinal cord to brain MRI in the routine follow-up of clinically stable relapsing-remitting patients with multiple sclerosis reveals a significant proportion of disease activity otherwise neglected, a fact that could have important implications in assessing and predicting treatment response [33&&]. However, these data need to be confirmed and should be taken with caution, as spinal cord MRI is more difficult to standardize and is probably less robust for assessing the presence of new T2 lesions, as compared to brain MRI. A recommended standardized spinal cord MRI protocol has been recently proposed by the MRI in Multiple Sclerosis (MAGNIMS) network [13& ].
CONTRIBUTION OF QUANTITATIVE MAGNETIC RESONANCE FOR ASSESSING SPINAL CORD DAMAGE
Spinal cord quantitative MRI techniques are emerging and seem to have great potential to improve the management of patients with multiple sclerosis (Table 3). As mentioned before, however, to date the use of these measures has provided new insights into the understanding of multiple sclerosis, but has shown limited clinical utility [34].
Conventional MRI clearly shows considerable spinal cord atrophy in multiple sclerosis, which represents the end-product of spinal cord disorder. As both axonal loss and demyelination can substantially reduce the cord volume, the MRI-based quantitative measurement of spinal cord cross-sectional area can be attractive as a potential pathological substrate of disability. This seems particularly true in patients with long-standing multiple sclerosis, where quantitative MRI studies have shown that reduced cord area is more pronounced and associated with increasing disability independently of brain changes [35,36]. Interestingly, however, a recent quantitative study has shown that significant atrophy and high structural variability is already present in the upper cervical cord at earliest stages of multiple sclerosis [37& ]. Longitudinal data support cross-sectional results, reporting higher spinal cord atrophy rates than brain rates (about 1.5 vs. 0.5 to 1% per year), highest in patients with secondary progressive multiple sclerosis (about 2% per year) and, more in general, higher in patients with worsening disability (about 2% per year) than in those with stable disease (about 1% per year) [38&&]. Recently, the development of semiautomated methods has provided a more rapid and reproducible measure of cord area than obtained with manual methods. Particularly, the active surface model [39] on three-dimensional PSIR images seems to improve the reproducibility of measurements and reduces the number of patients required for clinical trials using cord atrophy as an endpoint [40]. Finally, a voxel-based analysis of spinal cord atrophy has been attempted in some studies [41,42]. This can provide regional measures potentially able to differentiate the involvement of different cord areas in different multiple sclerosis Tab clinical phenotypes [42]. Voxel-based methods, however, rely greatly on accurate image registration, which is extremely challenging in the spinal cord and very difficult to be achieved on routine basis.
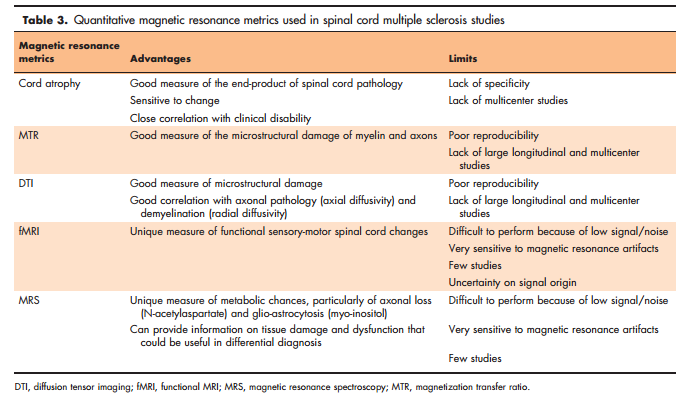
Although a global measure such as cord atrophy can approximate macroscopic tissue damage on MRI, measures of magnetization transfer and diffusion-weighted imaging can reveal the multiple sclerosis-associated microstructural abnormalities. Magnetization transfer imaging (MTI) is a quantitative MRI technique based on the continued interactions (e.g. exchange of magnetization) between the bulk of free water protons and the protons bound to macromolecules. The magnetization of bound protons can be saturated and transferred to the mobile protons with off-resonance radiofrequency pulse, thus reducing the signal intensity of the observable magnetization. The magnetization transfer ratio (MTR, calculated from the magnetization transfer saturated and unsaturated images) is the quantitative metric used to assess the magnitude of the magnetization transfer on tissues. Since in the central nervous system the bound protons are mainly associated with myelin and axonal membranes, the amount of signal decrease should indicate this nature of tissue damage. However, diffusion-weighted imaging evaluates both the diffusion of water molecules within a given structure (i.e. myelinated axons) and the diffusion of unrestricted water molecules. Because the magnitude of diffusion is dependent on the direction in which this is measured, a more complete characterization can be obtained from the diffusion tensor imaging (DTI). The latter provides parameters that might increase the specificity of MRI assessment by approximating multiple sclerosis pathological processes such as axonal loss (i.e. fractional anisotropy and axial diffusivity) and demyelination (i.e. radial diffusivity). Abnormalities in MTI and DTI measures of the cervical cord have been shown in several multiple sclerosis studies [11& ]. Overall, these studies showed that cord microstructural damage could be detected in patients with established multiple sclerosis, but not in those with clinically isolated syndromes [11& ]. Microstructural damage detected by both DTI and MTI changes result to be closely correlated with clinical measures [11& ]. More specifically, a recent study has shown that the microstructural abnormalities assessed by both MTI and DTI are more pronounced in patients with higher than in those with lower disability, with an increased sensitivity in comparison to conventional MRI measures [43]. More recently, a number of technical developments have been introduced to improve the analysis of both MTI and DTI data [11& ]. Indeed, an interesting metric has been developed that aims at overcoming the motion-related problems caused by the imperfect subtraction between saturated and unsaturated images and leading to an unreliable MTR. This metric assesses cord MTI by using only the magnetization-saturated image and measuring the signal at each voxel by dividing the voxel intensity by the intensity of the CSF (MTCSF imaging) [44]. In patients with multiple sclerosis, MTCSF measure has shown changes in the dorsal and in the lateral columns that were associated with sensorimotor impairment and clinical disability [45]. As for DTI, a voxel-based approach has been recently used on cervical spinal cord data of patients with multiple sclerosis [46] showing promising results despite the aforementioned limitations of the cord voxel-based approach.
Technical limitations challenge a wide use of functional MRI (fMRI) and proton magnetic resonance spectroscopy (MRS) of the spinal cord [47& ]. As in the brain, task-related fMRI experiments of the spinal cord have been based on the blood oxygenation level dependent (BOLD) principle. However, it is controversial if the activation seen during cord fMRI experiments can have the same origin of the BOLD contrast seen in the brain [48]. Despite this, task-related MRI activation of the spinal cord is feasible and, in multiple sclerosis studies, data report quite consistently increased activation in the spinal cord of patients with multiple sclerosis compared with healthy controls after sensory-motor tasks [49– 51]. More interesting results come from proton MRS studies of the spinal cord [47& ], as this technique is able to quantify a number of metabolites that can reveal specific cord-related abnormalities in multiple sclerosis. Proton MRS usually assesses myo-inositol, choline compounds, creatine and Nacetylaspartate (NAA). As in the brain, spinal cord levels of NAA (a reliable marker of axonal integrity) has shown consistently to be lower in multiple sclerosis patients than in healthy controls [52– 54]. In an interesting longitudinal study [55], spinal cord NAA levels partially recovered over time after a first decrease because of an acute relapse and this recovery predicted better clinical recovery. This suggests that in the spinal cord, as in the brain, NAA measures may reflect partially reversible axonal damage and dysfunction, possibly expression of mechanisms of tissue repair leading to clinical improvement [56]. Finally, a more recent proton MRS study [57] has demonstrated that low levels of myo-inositol normalized to creatine, possibly expression of astrocytic damage, can be found in the spinal cord lesions of patients with NMO when compared with the MRS pattern of the spinal cord lesions of patients with multiple sclerosis. This is in line with recent ex vivo evidence that NMO is an autoimmune astrocytopathy [58] and suggest that, if these preliminary data will be confirmed by new and larger studies, the in vivo quantification of myoinositol in the spinal cord may help in distinguishing NMO from multiple sclerosis.
CONCLUSION
Conventional spinal cord MRI is a valuable resource for assessing patients with multiple sclerosis because of its high sensitivity for depicting demyelinating lesions in this structure. Nonetheless, a meticulous procedure is essential to avoid artifacts and enable acquisition of high-quality images. Advanced quantitative techniques, in particular spinal cord atrophy, can measure the degree of tissue damage, providing a reliable assessment of the true burden of the disease. These techniques have the potential to provide clinically relevant markers of disease progression, but require validation prior to being considered as robust endpoints in clinical studies.
Acknowledgements
None.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDED READING
Papers of particular interest, published within the annual period of review, have been highlighted as: & of special interest && of outstanding interest
1. Lycklama G, Thompson A, Filippi M, et al. Spinal-cord MRI in multiple sclerosis. Lancet Neurol 2003; 2:555–562.
2. Stankiewicz JM, Neema M, Alsop DC, et al. Spinal cord lesions and clinical status in multiple sclerosis: a 1.5 T and 3 T MRI study. J Neurol Sci 2009; 279:99–105.
3. Philpott C, Brotchie P. Comparison of MRI sequences for evaluation of multiple sclerosis of the cervical spinal cord at 3 T. Eur J Radiol 2011; 80:780–785.
4. Bot JC, Barkhof F, Lycklama a` Nijeholt GJ, et al. Comparison of a conventional cardiac-triggered dual spin-echo and a fast STIR sequence in detection of spinal cord lesions in multiple sclerosis. Eur Radiol 2000; 10:753–758.
5. Riederer I, Karampinos DC, Settles M, et al. Double inversion recovery sequence of the cervical spinal cord in multiple sclerosis and related inflammatory diseases. Am J Neuroradiol 2015; 36:219–225.
6. Kober T, Granziera C, Ribes D, et al. MP2RAGE multiple sclerosis magnetic resonance imaging at 3 T. Invest Radiol 2012; 47:346–352.
7. Alcaide-Leon P, Pauranik A, Alshafai L, et al. Comparison of sagittal FSE T2, STIR, and T1-weighted phase-sensitive inversion recovery in the detection of spinal cord lesions in MS at 3T. Am J Neuroradiol 2016. [Epub ahead of print]
8. Schlaeger R, Papinutto N, Panara V, et al. Spinal cord gray matter atrophy correlates with multiple sclerosis disability. Ann Neurol 2014; 76:568–580.
9. Bot JC, Barkhof F, Polman CH, et al. Spinal cord abnormalities in recently diagnosed MS patients: added value of spinal MRI examination. Neurology 2004; 62:226–233.
10. Weier K, Mazraeh J, Naegelin Y, et al. Biplanar MRI for the assessment of the spinal cord in multiple sclerosis. Mult Scler 2012; 18:1560–1569.
11. & Gass A, Rocca MA, Agosta F, et al. MAGNIMS Study Group. MRI monitoring of pathological changes in the spinal cord in patients with multiple sclerosis. Lancet Neurol 2015; 14:443–454. This MAGNIMS review paper analyses the potential value of different magnetic resonance techniques (conventional and advanced) in assessing focal and diffuse damage of the spinal cord, which used in combination provides a better assessment of the true burden of disease.
12. & Kim HJ, Paul F, Lana-Peixoto MA, et al. MRI characteristics of neuromyelitis optica spectrum disorder: an international update. Neurology 2015; 84:1165–1173. This article summarizes the brain and spinal cord MRI findings of neuromyelitis optica spectrum disorders, which helps in distinguishing this condition from multiple sclerosis.
13. & Rovira A` , Wattjes MP, Tintore´ M, et al. MAGNIMS study group. Evidencebased guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis-clinical implementation in the diagnostic process. Nat Rev Neurol 2015; 11:471–482. The MAGNIMS study group have formulated these guidelines to better define and optimize the use of brain and spinal cord MRI in the diagnostic process of multiple sclerosis. These guidelines indicate that the added value of nonconventional magnetic resonance techniques in the diagnostic process remains to be established and requires further research.
14. Nijeholt GJ, van Walderveen MA, Castelijns JA, et al. Brain and spinal cord abnormalities in multiple sclerosis. Correlation between MRI parameters, clinical subtypes and symptoms. Brain 1998; 121:687–697.
15. Dalton CM, Brex PA, Miszkiel KA, et al. Spinal cord MRI in clinically isolated optic neuritis. J Neurol Neurosurg Psychiatry 2003; 74:1577–1580.
16. Okuda DT, Mowry EM, Cree BA, et al. Asymptomatic spinal cord lesions predict disease progression in radiologically isolated syndrome. Neurology 2011; 76:686–692.
17. Bot JC, Barkhof F. Spinal-cord MRI in multiple sclerosis: conventional and nonconventional MR techniques. Neuroimaging Clin N Am 2009; 19:81–99.
18. Thorpe JW, Kidd D, Moseley IF, et al. Serial gadolinium-enhanced MRI of the brain and spinal cord in early relapsing-remitting multiple sclerosis. Neurology 1996; 46:373–378.
19. Silver NC, Good CD, Sormani MP, et al. A modified protocol to improve the detection of enhancing brain and spinal cord lesions in multiple sclerosis. J Neurol 2001; 248:215–224.
20. Simon JH. The contribution of spinal cord MRI to the diagnosis and differential diagnosis of multiple sclerosis. J Neurol Sci 2000; 172 (Suppl 1):S32–S35.
21. Tartaglino LM, Friedman DP, Flanders AE, et al. Multiple sclerosis in the spinal cord: MR appearance and correlation with clinical parameters. Radiology 1995; 195:725–732.
22. Sombekke MH, Wattjes MP, Balk LJ, et al. Spinal cord lesions in patients with clinically isolated syndrome: a powerful tool in diagnosis and prognosis. Neurology 2013; 80:69–75.
23. Bot JC, Barkhof F, Lycklama a` Nijeholt G, et al. Differentiation of multiple sclerosis from other inflammatory disorders and cerebrovascular disease: value of spinal MR imaging. Radiology 2002; 223:46–56.
24. Tintore´ M, Rovira A, Arrambide G, et al. Brainstem lesions in clinically isolated syndromes. Neurology 2011; 75:1933–1938.
25. Cordonnier C, de Seze J, Breteau G, et al. Prospective study of patients presenting with acute partial transverse myelopathy. J Neurol 2003; 250:1447–1452.
26. Coret F, Bosca I, Landete L, et al. Early diffuse demyelinating lesion in the cervical spinal cord predicts a worse prognosis in relapsing-remitting multiple sclerosis. Mult Scler 2010; 16:935–941.
27. Rush CA, MacLean HJ, Freedman MS. Aggressive multiple sclerosis: proposed definition and treatment algorithm. Nat Rev Neurol 2015; 11:379– 389.
28. Menon S, Shirani A, Zhao Y, et al. Characterising aggressive multiple sclerosis. J Neurol Neurosurg Psychiatry 2013; 84:1192–1198.
29. Gholipour T, Healy B, Baruch NF, et al. Demographic and clinical characteristics of malignant multiple sclerosis. Neurology 2011; 76:1996–2001.
30. Filippi M, Rocca MA, De Stefano N, et al. Magnetic resonance techniques in multiple sclerosis: the present and the future. Arch Neurol 2011; 68:1514– 1520.
31. Tench CR, Morgan PS, Jaspan T, et al. Spinal cord imaging in multiple sclerosis. J Neuroimaging 2005; 15:94S–102S.
32. Wattjes MP, Rovira A, Miller D, et al. On behalf of the MAGNIMS study group. MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis – establishing disease prognosis and monitoring patients. Nat Rev Neurol 2015; 11:597–606.
33. && Zecca C, Disanto G, Sormani MP, et al. Relevance of asymptomatic spinal MRI lesions in patients with multiple sclerosis. Mult Scler 2015. [Epub ahead of print] This study shows that the identification of new asymptomatic spinal cord lesions is relatively frequent even in clinically stable relapsing-remitting multiple sclerosis patients, and contribute in predicting future disease course. These results support the value of adding spinal cord MRI to brain MRI in the follow-up of stable RRMS patients to monitor subclinical disease activity.
34. Wheeler-Kingshott CA, Stroman PW, Schwab JM, et al. The current state-ofthe-art of spinal cord imaging: applications. Neuroimage 2014; 84:1082– 1093.
35. Daams M, Weiler F, Steenwijk MD, et al. Mean upper cervical cord area (MUCCA) measurement in long-standing multiple sclerosis: relation to brain findings and clinical disability. Mult Scler 2014; 20:1860–1865.
36. Kearney H, Rocca MA, Valsasina P, et al. Magnetic resonance imaging correlates of physical disability in relapse onset multiple sclerosis of long disease duration. Mult Scler 2014; 20:72–80.
37. & Biberacher V, Boucard CC, Schmidt P, et al.Atrophy and structural variability of the upper cervical cord in early multiple sclerosis. Mult Scler 2015; 21:875–884. The study assessed onset of spinal cord atrophy in the disease course of multiple sclerosis showing that it may occur in the earliest stages of the disease.
38. && Lukas C, Knol DL, Sombekke MH, et al. Cervical spinal cord volume loss is related to clinical disability progression in multiple sclerosis. J Neurol Neurosurg Psychiatry 2015; 86:410–418. This is the first large, longitudinal study examining the temporal evolution of spinal cord atrophy in multiple sclerosis and its association with clinical progression. Results showed that progressive 24-month upper spinal cord atrophy occurs in all multiple sclerosis subtypes and is faster in patients exhibiting disease progression at month 24.
39. Horsfield MA, Sala S, Neema M, et al. Rapid semi-automatic segmentation of the spinal cord from magnetic resonance images: application in multiple sclerosis. NeuroImage 2010; 50:446–455.
40. Kearney H, Yiannakas MC, Abdel-Aziz K, et al. Improved MRI quantification of spinal cord atrophy in multiple sclerosis. J Magn Reson Imaging 2014; 39:617–623.
41. Valsasina P, Horsfield MA, Rocca MA, et al. Spatial normalization and regional assessment of cord atrophy: voxel-based analysis of cervical cord 3D T1-weighted images. Am J Neuroradiol 2012; 33:2195–2200.
42. Rocca MA, Valsasina P, Damjanovic D, et al. Voxel-wise mapping of cervical cord damage in multiple sclerosis patients with different clinical phenotypes. J Neurol Neurosurg Psychiatry 2013; 84:35–41.
43. Oh J, Saidha S, Chen M, et al. Spinal cord quantitative MRI discriminates between disability levels in multiple sclerosis. Neurology 2013; 80:540–547.
44. Smith SA, Golay X, Fatemi A, et al. Magnetization transfer weighted imaging in the upper cervical spinal cord using cerebrospinal fluid as intersubject normalization reference (MTCSF imaging). Magn Reson Med 2005; 54:201–206.
45. Zackowski KM, Smith SA, Reich DS, et al. Sensorimotor dysfunction in multiple sclerosis and column-specific magnetization transfer-imaging abnormalities in the spinal cord. Brain 2009; 132:1200–1209.
46. Toosy AT, Kou N, Altman DG, et al. Voxel-based cervical spinal cord mapping of diffusion abnormalities in MS-related myelitis. Neurology 2014; 83:1321– 1325.
47. & Kearney H, Miller DH, Ciccarelli O. Spinal cord MRI in multiple sclerosis – diagnostic, prognostic and clinical value. Nat Rev Neurol 2015; 11:327–338. This article summarizes quantitative MRI spinal cord studies on multiple sclerosis and discusses the new insights they have provided into the understanding of disease mechanisms.
48. Stroman PW, Wheeler-Kingshott C, Bacon M, et al. The current state-of-theart of spinal cord imaging: methods. Neuroimage 2014; 84:1070–1081.
49. Agosta F, Valsasina P, Rocca MA, et al. Evidence for enhanced functional activity of cervical cord in relapsing multiple sclerosis. Magn Reson Med 2008; 59:1035–1042.
50. Valsasina P, Agosta F, Absinta M, et al. Cervical cord functional MRI changes in relapse-onset MS patients. J Neurol Neurosurg Psychiatry 2010; 81:405– 408.
51. Valsasina P, Rocca MA, Absinta M, et al. Cervical cord FMRI abnormalities differ between the progressive forms of multiple sclerosis. Hum Brain Mapp 2012; 33:2072–2080.
52. Kendi AT, Tan FU, Kendi M, et al. MR spectroscopy of cervical spinal cord in patients with multiple sclerosis. Neuroradiology 2004; 46:764–769.
53. Ciccarelli O, Wheeler-Kingshott CA, McLean MA, et al. Spinal cord spectroscopy and diffusion-based tractography to assess acute disability in multiple sclerosis. Brain 2007; 130:2220–2231.
54. Marliani AF, Clementi V, Albini Riccioli L, et al. Quantitative cervical spinal cord 3T proton MR spectroscopy in multiple sclerosis. Am J Neuroradiol 2010; 31:180–184.
55. Ciccarelli O, Altmann DR, McLean MA, et al. Spinal cord repair in MS: does mitochondrial metabolism play a role? Neurology 2010; 74:721–727.
56. Ciccarelli O, Toosy AT, De Stefano N, et al. Assessing neuronal metabolism in vivo by modeling imaging measures. J Neurosci 2010; 30:15030–15033.
57. Ciccarelli O, Thomas DL, De Vita E, et al. Low myo-inositol indicating astrocytic damage in a case series of neuromyelitis optica. Ann Neurol 2013; 74:301–305.
58. Lucchinetti CF, Guo Y, Popescu BF, et al. The pathology of an autoimmune astrocytopathy: lessons learned from neuromyelitis optica. Brain Pathol 2014; 24:83–97.
