Influence of Spasticity on Mobility and Balance in Persons With Multiple Sclerosis

Selected By
June Halper, MSN, APN-C, MSCN, FAAN
Why is this important to me?
Spasticity refers to muscle stiffness, involuntary muscle movement, and sudden movements. Around 80% of people with MS report spasticity, and it most commonly affects the lower limbs. Spasticity in the legs likely affects balance, mobility, and posture control. This study addressed the question of whether people with MS with spasticity in the lower limbs have worse mobility and balance than people with MS without spasticity.
What is the objective of this study?
Compared to the group without spasticity, the group with spasticity had more severe disability and more balance problems. Also, their mobility was more impaired.
This conclusion may seem obvious, but the authors wanted to shed some light on an interesting issue in treating spasticity. Previous work has shown that drugs such as baclofen that reduce spasticity do not improve mobility or disability in people with MS. If treating spasticity does not improve problems with mobility or disability, then many healthcare providers have wondered if the decreased mobility and balance in the group with spasticity may not be a direct result of spasticity. Instead, the spasticity group may have had greater impairment in muscle strength, sensation, or range of motion that led to the mobility and balance problems independent of spasticity.
Spasticity, mobility, and disability progression interact in complex ways in MS. No cause-and-effect relationship could be determined between spasticity and the other factors measured. Whether spasticity causes mobility and balance problems independent of MS-related disability is unknown and requires future studies.
Interestingly, rehabilitation programs aimed at improving mobility and balance also improve spasticity. Caution is required, however, before beginning a program aimed at improving spasticity. Sometimes reducing spasticity can lead to a loss in mobility because spasticity increases the muscle tone needed for walking and balance. Future studies should look for therapeutic interventions that reduce spasticity and also improve mobility and balance.
How did the authors study this issue?
The authors studied 34 people with MS, 22 of whom were women. Participants were an average age of 57 years and lived in Utah. Patients were evaluated for spasticity and a variety of walking and balance tests. Fifteen participants had spasticity and 19 did not.
Original Article
Influence of Spasticity on Mobility and Balance in Persons With Multiple Sclerosis
Journal of Neurologic Physical Therapy
Jacob J. Sosnoff, PhD, Eduard Gappmaier, PT, PhD, Amy Frame, PT, and Robert W. Motl, PhD
INTRODUCTION
Spasticity is defined as a motor disorder characterized by a velocity-dependent increase in tonic stretch reflexes and exaggerated tendon reflexes resulting from increased excitability of the stretch reflex.1 Spasticity is often observed in individuals with pathology of the motor areas of the central nervous system (CNS). Indeed, spasticity has been reported by more than 80% of persons with multiple sclerosis (MS) and is most prevalent in the lower limbs.2 The presence of spasticity in the lower limbs likely affects mobility and balance in persons with MS.3,4 Evidence from the North American Research Committee on MS4 indicates that self-reported spasticity was associated with mobility impairments. There is additional evidence of an association between lower limb spasticity and postural control dysfunction in persons with MS.5 Collectively, there have been very few direct examinations of the influence of spasticity on mobility and balance in persons with MS. Recent evidence indicates that the presence of spasticity in upper and lower limbs of persons with MS results in worse performance on the 6-minute walk test (6MWT) compared with the absence of spasticity.6 Nevertheless, this study did not include other mobility or balance tasks as outcome measures, and spasticity was not isolated to the lower extremities.6 As such, the influence of lower limb spasticity on mobility and balance in persons with MS has not been well-characterized. The current study examined the hypothesis that persons with MS who had spasticity of the lower limbs would have more impairment of mobility and balance performance than persons with MS who did not have spasticity.
METHODS
Participants
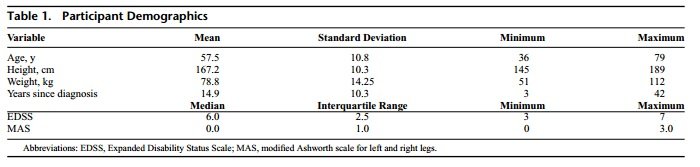
The sample included 34 participants (22 women) from the University of Utah Multiple Sclerosis Rehabilitation and Wellness Program who underwent mobility and spasticity assessments as part of an annual physical therapy evaluation. All participants signed a consent form approved by the University of Utah Institutional Review Board. Participants were ambulatory, had a diagnosis of definite MS, and ranged in age from 36 to 79 years with a mean of 57 years (SD = 10.6 years). The average time since diagnosis was 16.5 years (SD = 9.9 years) and ranged between 3 and 33 years.
The study sample had a range of expanded disability status scale (EDSS) scores between 3.5 and 7.0, an interquartile range of 2.25 with a median 6.0. The EDSS is a disability scale based on the function of 8 different systems including the pyramidal, cerebellar, brain stem, sensory, bowel and bladder, visual, mental, and other.7 Expanded disability status scale scores range from 0 to 10, with 0 representing no neurological impairment, 2.0 representing minimal disability in one functional system, 4.0 reflecting the onset of walking impairment, 6.0 corresponding to the requirement of unilateral assistance (eg, cane or crutch), 8.0 indicating that the individual is unable to walk and is restricted to bed, and 10.0 indicating death due to MS.
The range of modified Ashworth scale (MAS) scores for the right and left legs were between 0 and 2 and 0 and 3, respectively, where 0 = no increase in muscle tone, and 4 = the affected part is rigid. The interquartile range was 1.0 and the median was 0.0 for both legs. Participants with MAS scores 1.0 or more for either leg were classified as being in the spasticity group (n = 15), whereas the participants with MAS scores less than 1.0 were classified as being in the no spasticity group (n = 19). Of the participants in the spasticity group, 3 had unilateral spasticity (2 right leg), and 12 had bilateral spasticity.
Procedures
Participants underwent an EDSS evaluation by a clinician and measurement of spasticity in the gastroc-soleus muscles of both legs using the MAS8 by a physical therapist. Multiple measures of mobility were used, walking speed was assessed using the timed 25-foot walk (T25FW; 7.6 m),9 upright mobility was measured using the Timed Up and Go (TUG),10 walking endurance was measured using the 6MWT, and self-reported impact of MS on walking ability was assessed using the Multiple Sclerosis Walking Scale-12 (MSWS-12).11 Balance was measured with the Berg Balance Test (BBT)12 and Activities-specific Balance Confidence Scale (ABC).13
Statistical Analysis
All analyses were completed using SPSS version 17.0 (SPSS Inc, Chicago, Illinois) and significance was accepted at P < 0.05. Between-group difference in mobility and balance were examined using independent samples t tests. Differences between spasticity groups in EDSS scores were examined using the nonparametric Mann-Whitney U test. To determine whether the influence of spasticity on mobility and balance was simply a result of greater disability in the spasticity group, Spearman rank correlation coefficients (ρ) were calculated. To determine whether mobility influenced the association between spasticity and disability, partial correlations controlling for mobility (ie, T25FW, TUG, 6MWT) were conducted. Effect sizes based on a difference in mean scores were expressed as Cohen’s d. 14
RESULTS
There were no differences between groups in height, weight, time since diagnosis or age (P = 0.68), but there was a between-group difference in EDSS (P = 0.03). The spasticity group had a greater EDSS (median score = 6.0, range = 3.5- 6.5) than the no spasticity group (median score = 4.0, range = 3.0-6.5), indicating greater disability in the spasticity group.
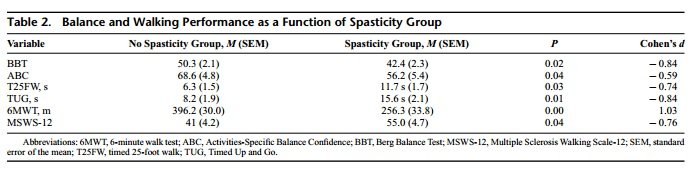
The spasticity group had significantly worse balance performance (BBT, P = 0.02) and self-reported balance ability (ABS, P = 0.04). Overall, the difference was moderate to large in magnitude based on effect sizes for BBT (d = − 0.84) and ABC scores (d = − 0.59) (see Table 1).
The spasticity group also had more impaired mobility as indexed by the T25FW (P = 0.02), TUG (P = 0.01), 6MWT distance (P < 0.01), and MSWS-12 (P = 0.04) (see Table 2). Overall, the differences were moderate to large in magnitude based on effect sizes for T25FW (d = − 0.74), TUG (d = − 0.84), 6MWT (d = 1.03), and MSWS-12 (d = − 0.76).
A significant correlation between EDSS and MAS scores for the left and right ankle was found (ρ = 0.39 and 0.37, respectively; P < 0.05 for each). It is important to note that the association between EDSS and MAS was not significant when controlling for mobility measures (ρ = − 0.03 and − 0.02, respectively; P > 0.05 for each). Overall, these results suggest a complex interaction between spasticity, mobility, and disability progression.
DISCUSSION
The primary contribution of the current study was that persons with lower limb spasticity had worse mobility and balance as indexed by performance tasks and self-reported measures than those without spasticity. However, this relationship must be interpreted with caution in the present study sample, as the group with spasticity also had a higher median EDSS score than those without spasticity, suggesting greater overall disability in the spasticity group. The significant correlation between EDSS and MAS scores for both lower extremities suggest that the two constructs are related in some way, but the nature of this relationship is unknown. Whether spasticity contributes to disability or is the consequence of disability is not known. While we are unable to offer insights into this relationship given the design of the present study, in a subsequent section we will explore this issue further.
Our findings are consistent with previous research wherein persons with MS who had spasticity had greater selfreported disability,2 6MWT distance,6 balance,5 and falls.15
This literature underscores the importance of future studies to determine whether spasticity causes mobility and balance impairment independent of the state of MS-related disability. The nature of this relationship is puzzling, as antispastic pharmacological agents (such as baclofen) are effective for reducing spasticity, but have not been shown to have a beneficial effect on mobility and disability outcomes in individuals with MS.16 Perhaps antispastic agents reduce spasticity but interfere with motor control processes involved in mobility and postural control, and this might be avoided with rehabilitation approaches such as exercise and physical therapy. If it is shown that spasticity contributes to impairment, then it will be important to examine rehabilitation approaches for managing spasticity as a method for improving mobility and balance in MS. To that end, clinicians and patients would benefit from additional research to identify alternative approaches for managing spasticity that have secondary beneficial effects on mobility and balance.
The current observations are congruent with a recent report demonstrating that persons with MS who have spasticity of the upper and lower limbs (based on MAS scores) performed more poorly on the 6MWT than those without spasticity.6 The current investigation extended that research, demonstrating that persons with MS with spasticity have worse performance not only on tests of walking endurance (eg, 6MWT distance) but also on shorter walking tasks (eg, 25FTW and TUG) and self-reports of walking impairment (eg, MSWS-12 scores) as well as clinical and self-reports of balance (eg, ABC and BBT). It is of interest to examine whether other aspects of mobility such as free living walking17 are influenced by spasticity in persons with MS.
The current results are not consistent with reports in other neurologic clinical populations, which have shown no association between spasticity and mobility impairment in persons with stroke18 or cerebral palsy.19,20 A possible explanation for this inconsistency is differences among studies in the measure used to quantify spasticity. The studies of other clinical populations (cited earlier) utilized dynamometry to quantify spasticity, rather than the MAS that used in the current and previous research in MS.6 Researchers might consider further examining the effect of spasticity on mobility and balance across patient populations by using a standard set of outcomes for documenting the specificity or generalizability of any effect of spasticity on mobility or balance and the effects of rehabilitation interventions.
As noted previously, the median EDSS score was significantly greater in the spasticity group than the group without spasticity. The emphasis on walking ability in determining EDSS scores, particularly in the middle range of scores (4.0- 6.5),20 provides some basis for the result that those in the spasticity group had greater impairment of mobility and elevated EDSS scores. It is possible that the difference in EDSS scores between groups can be explained by the influence of spasticity itself on disability.21 Indeed, the items on the EDSS which most closely reflect pyramidal tract function (ie, the pyramidal functional score) are mainly determined by reflex function [eg, spasticity]) and have the strongest association with the total EDSS score.21 The significant association between spasticity and disability progression observed in the current investigation is congruent with this notion. Alternatively, the influence of spasticity on between-group differences in EDSS scores might be driven by mobility impairment. The observation that the association between spasticity and EDSS is minimized when mobility is controlled for strengthens this possibility. Obviously, further research should explore the link among EDSS scores, spasticity, and mobility in MS.
It is also possible that the decreased mobility and balance in the spasticity group was not the direct result of lower limb spasticity but rather that the spasticity group had greater impairment in other factors (eg, muscle strength, proprioception, range of motion) that contribute to mobility and balance impairments. Unfortunately, data on other factors were not collected in the current investigation. Ultimately, larger studies wherein there is control for possible contributing factors are needed to determine whether spasticity is uniquely associated with mobility and balance impairment in persons with MS.
Clinical judgment might suggest that the reduction of spasticity should result in improved mobility and balance. Indeed, rehabilitation programs that have lead to improve mobility and balance have typically documented reductions in spasticity in persons with MS.22 It is important to note that although the pilot investigation of Giesser and colleagues22 demonstrated improvements in mobility, balance, and spasticity, a causal relationship cannot be inferred. Evidence that a reduction in spasticity will result in improved mobility and postural control is lacking.16 Furthermore, caution should be taken before applying interventions intended to reduce spasticity in some persons with MS; a reduction of spasticity might result in a loss of mobility, because spasticity increases the muscle tone necessary for walking and balance.23 Additionally, future work should examine the conditions and modalities whereby reductions in spasticity manifest as improvements in mobility and balance in subjects with MS.
LIMITATIONS
The most important limitation in the current investigation is that spasticity was assessed while the subjects were at rest and not during walking or balance tasks. Because re- flexes are dependent on limb position and the task,24 spasticity should be assessed during mobility and balance tasks in future investigations. Additional limitations include a relatively small sample and lack of an objective measure of spasticity. Nevertheless, our findings are noteworthy by providing empirical evidence that persons with MS who have lower limb spasticity exhibit greater mobility and balance impairments than those without spasticity.
CONCLUSIONS
Overall, this investigation revealed that spasticity in the gastroc-soleus muscles appears to have negative effect on numerous aspects of mobility (walking speed, endurance, and self-reported walking impairment) and balance in persons with MS. Further research is needed to determine the complex interaction between spasticity, mobility, and disability in persons with MS.
REFERENCES
1. Lance JW. The control of muscle tone, reflexes, and movement: Robert Wartenberg lecture. Neurology. 1980;30(12):1303-1313.
2. Rizzo MA, Hadjimichael OC, Preiningerova J, Vollmer TL. Prevalence and treatment of spasticity reported by multiple sclerosis patients. Mult Scler. 2004;10(5):589-595.
3. Sinkjaer T, Andersen JB, Nielsen JF. Impaired stretch reflex and joint torque modulation during spastic gait in multiple sclerosis patients. J Neurol. 1996;243(8):566-574.
4. Johnson GR. Outcome measures of spasticity. Eur J Neurol. 2002;9:10-16.
5. Sosnoff JJ, Shin S, Motl RW. Multiple sclerosis and postural control: the role of spasticity. Arch Phys Med Rehabil. 2010;91(1):93-99.
6. Kuspinar A, Andersen RE, Teng SY, Asano M, Mayo NE. Predicting exercise capacity through submaximal fitness tests in persons with multiple sclerosis. Arch Phys Med Rehabil. 2010;91(9):1410-1417.
7. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11): 1444-1452.
8. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987;67(2):206-207.
9. Kaufman M, Moyer D, Norton J. The significant change for the Timed 25-foot Walk in the multiple sclerosis functional composite. Mult Scler. 2000;6(4):286-290.
10. Nilsagard Y, Lundholm C, Gunnarsson LG, Dcnison E. Clinical relevance using timed walk tests and ‘timed up and go’ testing in persons with multiple sclerosis. Physiother Res Int. 2007;12(2):105-114.
11. Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ. Measuring the impact of MS on walking ability: the 12-Item MS Walking Scale (MSWS-12). Neurology. 2003;60(1):31-36.
12. Berg KO, Maki BE, Williams JI, Holliday PJ, Wood-Dauphinee SL. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil. 1992;73(11):1073-1080.
13. Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci. 1995;50A(1):M28-34.
14. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 3rd ed. New York, NY: The Academies Press; 1988.
15. Nilsagard Y, Denison E, Gunnarsson LG, Bostrom K. Factors perceived as being related to accidental falls by persons with multiple sclerosis. Disabil Rehabil. 2009;31(16):1301-1310.
16. Orsnes GB, Sorensen PS, Larsen TK, Ravnborg M. Effect of baclofen on gait in spastic MS patients. Acta Neurol Scand. 2000;101(4):244-248.
17. Sosnoff JJ, Goldman MD, Motl RW. Real-life walking impairment in multiple sclerosis: preliminary comparison of four methods for processing accelerometry data. Mult Scler. 2010;16(7):868-877.
18. Ada L, Vattanasilp W, O’Dwyer NJ, Crosbie J. Does spasticity contribute to walking dysfunction after stroke? J Neurol Neurosurg Psychiatry. 1998;64(5):628-635.
19. Crenna P. Spasticity and “spastic” gait in children with cerebral palsy. Neurosci Biobehav Rev. 1998;22(4):571-578.
20. Ross SA, Engsberg JR. Relationships between spasticity, strength, gait, and the GMFM-66 in persons with spastic diplegia cerebral palsy. Arch Phys Med Rehabil. 2007;88(9):1114-1120.
21. Kurtzke JF. Historical and clinical perspectives of the expanded disability status scale. Neuroepidemiology. 2008;31(1):1-9.
22. Giesser B, Beres-Jones J, Budovitch A, Herlihy E, Harkema S. Locomotor training using body weight support on a treadmill improves mobility in persons with multiple sclerosis: a pilot study. Mult Scler. 2007;13(2): 224-231.
23. Kesselring J, Beer S. Symptomatic therapy and neurorehabilitation in multiple sclerosis. Lancet Neurol. 2005;4(10):643-652. 24. Stein AB, Yang JF, Belanger M, Pearson KG. Modification of reflexes in normal and abnormal movements. In: Allum JHJ, Allum-Mecklenburg DJ, Harris FP, eds. Progress in Brain Research. Vol 97. Amsterdam, the Netherlands: Elsevier; 1993:189-196.